
The COVID-19 pandemic has had a seismic impact on the UK healthcare system, driving the reorganisation and redistribution of services on a hitherto unseen depth and scale, and mandating a flexible and pragmatic approach towards the delivery of acute healthcare under unpredictable service pressures (Anderson et al, 2020). In particular, it has been difficult to determine optimal frontline clinical management in frail, elderly patients as their vulnerability to infection, their high mortality risk and the concomitant need for careful investigation and timely administration of supportive therapy has to be weighed against the risks of admission to secondary care institutions with high risk of nosocomial COVID-19 transmission (British Geriatric Society, 2021).
Before the COVID-19 pandemic, pressures on the NHS were already widespread and well described (NHS, 2019). Key approaches to tackling the growing demand for acute medical services have included the reconfiguration of acute-care pathways to provide a more flexible, efficient, patient-centred approach to clinical care, with an increased emphasis on extending acute healthcare services to community and home settings, and collaborative working across traditional organisational divides (NHS, 2019; Inada-Kim et al, 2020).
Access to rapid-turnaround diagnostic technologies such as point-of care testing (POCT) has been a critical component of this approach. POCT has become increasingly part of routine clinical practice in emergency department and ambulatory care settings, in addition to the use of early senior decision-making and increased access to imaging (Jones et al, 2016).
The diagnostic performance and reliability of such tests has already been validated in elderly patients in a community setting (Verbakel et al, 2020). Community diagnostic units have provided considerable benefits in ambulatory care for frail elderly patients in terms of better outcomes and patient experience, along with a reduced burden on acute services. However, the transport needs of patients with reduced mobility can often preclude them from accessing these services.
Transporting dependent patients with frailty syndromes to and from hospital often requires significant resources from an already-overstretched ambulance service. It can be extremely difficult to achieve on a same-day basis, with the concomitant risks of overnight stay in overburdened acute medical units, the breakdown in existing home care and risks of hospital-acquired diseases such as infection (including COVID-19), deconditioning and thromboembolism (Dharmarajan et al, 2020).
Hospital-at-home services have the capacity to deliver much of the patients' treatment in a home setting, though these services are typically implemented only after an initial, more comprehensive assessment, usually in a hospital or community diagnostic unit (Caplan et al, 2012).
Studies determining the utility of POCT in the assessment of frail patients in the prehospital setting, however, have previously shown only modest benefits, with limitations centred around poor practitioner uptake, governance issues and clinicians being unfamiliar with using blood test results in decision-making.
To date, these studies have focused primarily on the introduction of point-of-care tests for clinical biomarkers that are well established in acute secondary care (e.g. urea and electrolytes) into the clinical assessments of professional groups such as paramedics and GPs who have not habitually incorporated these into their decision-making when dealing with acutely unwell patients (McPherson, 2019; Hayward et al, 2020).
A more recent study, however, concerning the activities of a combined physician and occupational therapy service in Dublin, has suggested there is potential for a significantly larger benefit in terms of admission prevention when diagnostic and therapeutic resources are directed to frail patients in a prehospital setting. It reported a non-conveyance rate of 92%, although the paper lacks significant granular clinical detail of the nature of cases attended (McNamara et al, 2020).
Aim
This pilot study evaluated a prototype service, which included immediate telephone decision support from senior physicians in paramedic assessments of frail patients in supportive care environments that had been enhanced by point-of-care testing. The study aimed to assess the potential utility of this service in facilitating alternatives to hospital admission.
Method
To establish the prototype frailty response unit, a single rapid response vehicle was equipped with Abbott i-STAT point-of-care-testing enhanced by a novel wireless technology that could transmit results directly to the hospital Electronic Patent Record (EPR) system (Figures 1and2).


This vehicle was staffed on a rota by specialist paramedics, and was dispatched to frail, non-injured patients as identified by 999 call handlers over a 3-month period.
The term ‘specialist paramedics’ in this report describes band 7 paramedics who have had an additional 2 years' education and training leading to higher-level assessment and management skills, and who are able to diagnose a wider range of conditions and treat many minor injuries and illnesses, but do not routinely assess blood test results. They are, however, able to signpost care, and refer patients to professionals in the community such as GPs, community nurses or social care practitioners, and can also refer patients to hospital specialists, avoiding conveyance to emergency departments.
The paramedics involved in the project all attended a 1-hour training session before the project started to familiarise themselves with the study criteria, and to allow them to acquire skills in taking and handling blood samples using the i-STAT platform.
There was no funding for dedicated staff for this project and, because of the limitations of staffing and service demands, the service was deployed only on an ad-hoc basis when trained staff were available.
Patient selection and assessment
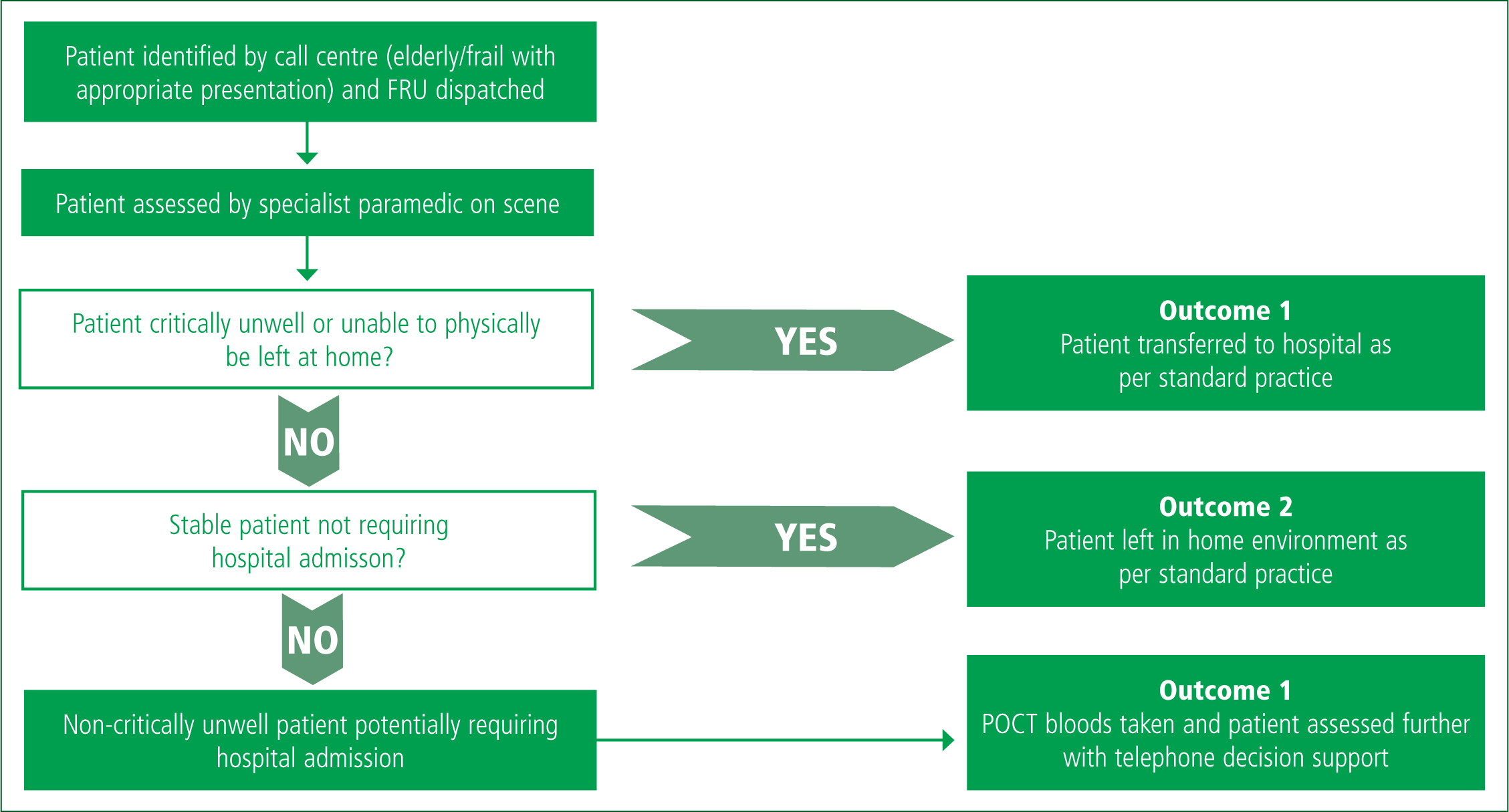
The screening process is summarised in Figure 3. Potential patients for inclusion were identified by the 999 call handlers in the clinical coordination centre as requiring more detailed clinical assessment than that which would typically be offered by community response teams (e.g. occupational therapy or physiotherapy), and selected using the criteria:
Where multiple calls for potentially suitable patients occurred at the same time, priority was given to people known to have a strong care support environment, such as a nursing home, a care home, having a 24-hour carer or living with or near to supportive family.
Potentially suitable patients were then assessed by the paramedic on scene with one of three outcomes:
Therefore, only non-critically unwell frail or elderly patients who were deemed to require transfer to secondary care were enrolled (outcome 3).
Clinical biochemistry results (Table 1) obtained on scene for the enrolled patients were transmitted to the hospital EPR system. The paramedic then discussed the patient with a senior physician in an acute medical assessment unit by telephone for decision support as to the optimal next steps for care, and to help coordinate referral to secondary care or other services if required.
| Characteristic | All patients (n=56) | Transferred patients (n=27) | Non-transferred patients (n= 29) |
|---|---|---|---|
| Median age (IQR) | 86 (79–90) | 87 (80–90) | 86 (79–90) |
| Sex: Male | 21 | 11 | 10 |
| Sex: Female | 35 | 16 | 19 |
| Median NEWS2 (IQR) | - | 3.5 (2.8–5.0) | - |
| Point-of-care testing results: cartridge 1: (CG4+) | |||
| Mean pH (7.35–7.45) | 7.41 (±0.05) | 7.41 (±0.06) | 7.41 (±0.05) |
| Number of patients with abnormal pH (<7.35 or >7.45) | 8 | 6 | 2 |
| pH range | 7.26–7.53 | 7.26–7.53 | 7.33–7.51 |
| Mean base excess (mmol/litre) (–2.0 to 2.0) | 1.37 (±4.55) | 1.36 (±5.2) | 1.4 (±4.0) |
| Number of patients with abnormal base excess | 26 | 12 | 14 |
| Base excess range (mmol/litre) | –10 to 13 | –10 to 13 | –10 to 5 |
| Mean bicarbonate (mmol/litre) (22–26) | 26.1 (±4.4) | 26.1 (±5.1) | 26.1 (±3.98) |
| Number of patients with abnormal bicarbonate | 28 | 13 | 15 |
| Bicarbonate range (mmol/litre) | 13.6–34.1 | 16.5–35.2 | 13.6–34.1 |
| Mean lactate (mmol/litre) (0.36–1.25) | 1.54 (±0.77) | 1.57 (±0.74) | 1.51 (±0.81) |
| Number of patients with lactate >2.0 | 8 | 5 | 3 |
| Lactate range (mmol/litre) | 0.41–4.88 | 0.41–3.36 | 0.79–4.88 |
| Point-of-care testing results: cartridge 2: (Chem 8) | |||
| Mean anion gap (mmol/litre) (10–20) | 15.2 (±2.7) | 15.8 (±3.0) | 14.7 (±2.5) |
| Number of patients with abnormal anion gap | 1 | 0 | 1 |
| Anion gap range (mmol/litre) | 10–21 | 10–20 | 10–21 |
| Mean urea (mmol/litre) (2.8–9.3) | 9.0 (±6.6) | 10.1 (±9.3) | 8.0 (±3.5) |
| Number of patients with abnormal urea | 17 | 10 | 7 |
| Urea range (mmol/litre) | 2.8–44.9 | 2.8–44.9 | 3.1–20.4 |
| Mean ionised calcium (mmol/litre) (1.12–1.32) | 1.18 (±0.08) | 1.15 (±0.09) | 1.2 (±0.06) |
| Number of patients with abnormal ionised calcium | 6 | 5 | 1 |
| Calcium range (mmol/litre) | 0.86–1.39 | 0.86–1.39 | 1.08–1.31 |
| Mean chloride (mmol/litre) (98–109) | 100 (±6.4) | 98.2 (±6.7) | 102 (±5.9) |
| Number of patients with abnormal chloride | 17 | 10 | 7 |
| Chloride range (mmol/litre) | 83–117 | 83–109 | 92–117 |
| Mean creatinine (mmol/litre) (53–114) | 103 (±64.5) | 121 (±83.7) | 88.8 (±41.6) |
| Number of patients with abnormal creatinine | 13 | 9 | 4 |
| Creatinine range (mmol/litre) | 45–318 | 45–318 | 48–252 |
| Mean glucose (mmol/litre) (3.9–5.8) | 6.8 (±2.3) | 6.4 (±2.1) | 7.1 (±2.4) |
| Number of patients with abnormal glucose | 30 | 9 | 21 |
| Glucose range (mmol/litre) | 2.1–15.7 | 3.3–11.3 | 2.1–15.7 |
| Mean potassium (mmol/litre) (3.5–4.9) | 4.1 (±0.8) | 3.9 (±1.0) | 4.2 (±0.60) |
| Number of patients with abnormal potassium | 9 | 5 | 4 |
| Potassium range (mmol/litre) | 2.8–7.8 | 2.8–7.8 | 3.0–5.8 |
| Mean sodium (mmol/litre) (138–146) | 135 (±6.9) | 136 (±6.0) | 137 (±5.1) |
| Number of patients with abnormal sodium | 7 | 6 | 1 |
| Sodium range (mmol/litre) | 121–155 | 121–147 | 129–155 |
| Mean total carbon dioxide (mmol/litre) (23–27) | 25.9 (±4.2) | 25.9 (±5.0) | 25.9 (±3.7) |
| Number of patients with abnormal total carbon dioxide | 25 | 12 | 13 |
| Carbon dioxide range (mmol/litre) | 14–37 | 18–37 | 14–33 |
Based on the outcome of the discussion, a decision was made to:
Tests
Standard, commercially available cartridges (CG4+ and Chem 8) were used on the Abbot i-STAT platform. These measure a range of parameters equivalent to standard laboratory venous blood gas with lactate, urea and electrolytes, glucose and ionised calcium (Table 1). These were chosen as they are already well validated in acute hospital settings and are in widespread clinical use, and cover a wide range of routinely measured parameters in acutely unwell patients.
Results were transmitted to the hospital EPR via the Abbott i-STAT 1 wireless platform using a dedicated virtual private network (VPN); approval for this had already been obtained through the trust's information governance process.
Immediate decision support was available via a pre-existing telephone referral/advice service staffed by senior hospital physicians (acute general medical consultants and registrars) working in the ambulatory assessment unit from 8:00 am–9:00 pm Monday to Friday and 10:00 am–7:00 pm on Saturday and Sunday.
Patient demographics, care environment, i-STAT results, disposition, decision to admit, subsequent diagnoses and admission parameters were obtained retrospectively from EPR by the study team. Any unplanned hospital admissions over the following 30 days were also identified and recorded.
Mean values were calculated for each i-STAT assay and overall length of stay if admitted, and median values calculated for the patient cohort's age and National Early Warning Score (NEWS2) score based on their initial observations.
Results
The project ran from 1 April to 30 June 2019 (91 days altogether). A total of 103 patients were visited and assessed by the South Central Ambulance Service frailty response unit during this period following dispatch from the central call centre.
From this group, 61 patients were selected by the paramedic based on the eligibility criteria for point-of-care testing (outcome 3), with 42 patients being deemed either critically unwell or not in need of secondary care assessment (outcome 1 or 2). Five patients were not identifiable in the EPR from the information given, leaving 56 patients for analysis (21 men and 35 women with a median age of 86 years (IQR 79–90)).
No patients declined blood tests, all samples were reported as successfully processed and all results from bloods taken were successfully transmitted to their hospital EPR, as South Central Ambulance Service staff reported. Fifty-five out of the 56 patients had at least one blood test result outside the normal reference range.
The results for tested patients are summarised in Figure 4. Overall, there was no significant difference in the number and range of abnormal tests between the transferred and the non-transferred cohorts as determined by POCT (Table 1). Fifteen of the 26 transferred patients were found to have a significantly elevated C-reactive protein or white cell count on admission to hospital. Concordance between POCT and lab blood tests of patients transferred to hospital was high.
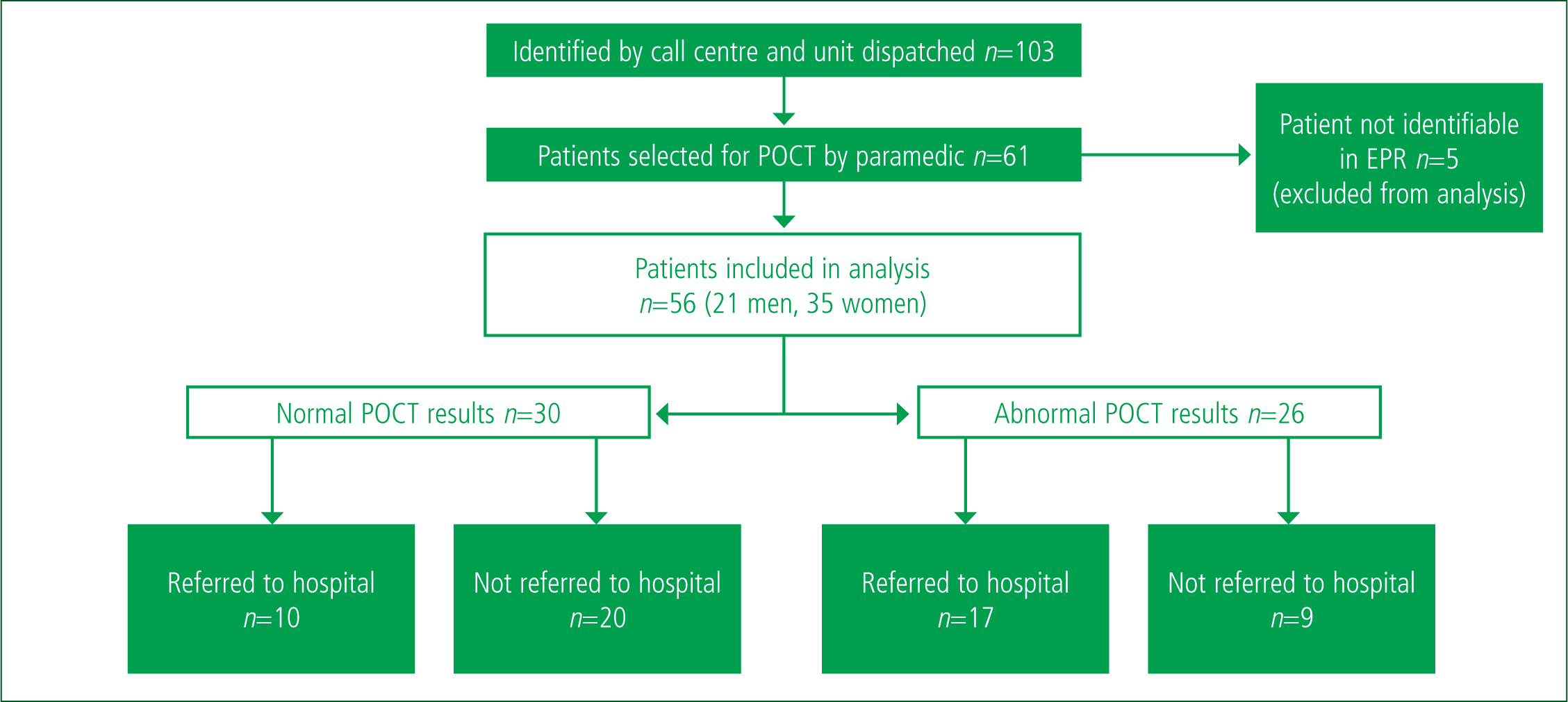
Out of the 56 patients enrolled, 27 were transferred for further assessment in hospital. Of these, 17 had significantly deranged blood tests, and 10 patients conveyed did not have significantly deranged blood tests. Twenty-nine patients remained in their usual care environment; of these, four patients presented to hospital within the next 30 days, with no deaths or reported adverse events as a consequence of non-conveyance recorded.
Eleven of the transferred patients had deranged observations on admission to hospital, with a median NEWS2 score of 3.5 (IQR 2.8–5.0).
Admitted patients received a wide range of discharge diagnoses, including small bowel obstruction, urosepsis, myocardial infarction, metastatic cancer and sepsis. Twenty-two patients underwent imaging during their admission, with nine undergoing cross-sectional imaging (computerised tomography (CT) of the head, CT of the chest, abdomen, and pelvis, CT pulmonary angiogram or magnetic resonance imaging of the head) before discharge (Table 2). The median length of stay in the transferred cohort was 2 days (IQR 1.5–12.5).
| Intervention/outcome | Number of transferred patients receiving intervention |
|---|---|
| Radiology | |
| Chest x-ray | 12 |
| Computerised tomography | 9 |
| Other | 3 |
| Treatment | |
| Intravenous fluids | 22 |
| Antibiotics | 18 |
Discussion
The results from this pilot study provide evidence to suggest that point-of-care blood testing is feasible within the ambulance service and, when combined with senior decision support, may allow a proportion of older adults who are frail and acutely ill to remain at home.
Regional figures suggest that paramedic crews in the region attend more than 600 calls per month for falls, with around 50% of paramedic contacts resulting in conveyance to secondary care in this population (unpublished data).
The people included in this study were drawn from a population that would typically have been conveyed to hospital, but a high proportion (29 out of 56 (52%)) of those who were initially identified as needing hospital admission were managed successfully at home following further assessment with blood tests and senior physician support. Although three out of 29 patients (10%) later attended a secondary care assessment, no adverse events were identified and, in two cases, no further treatment was required on the subsequent visit.
The study population included a heterogenous mix of older patients, with a range of underlying pathologies. Those admitted exhibited a range of clinical complexity and acuity, as evidenced by the widespread need for further imaging (including cross-sectional imaging) on attendance at hospital, the ranges of the median NEWS2 score and the variety of discharge diagnoses on hospital records.
The extended length of stay in the admitted group compared to the relatively low number of patients later presenting to hospital in the non-transferred group suggests that the overall assessment process was effective in discriminating between patients who required admission and those who could be safely left in their own home.
The even distribution of abnormal blood tests across the two groups indicate that using these measurements alone would not be sufficient to guide referral to secondary care, and that clinical decision-making and decision support may have played a significant part in decisions to transfer to hospital.

A high concordance between lab and POCT measurements and the 100% wireless transmission rate from the i-STAT units indicate this approach provides a robust and reliable method for obtaining results.
Previous studies looking at the use of POCT without additional clinical decision support in this clinical scenario have shown it has little effect on conveyance rate (McPherson, 2019; Hayward et al, 2020). In the evaluation described here, the likelihood of admission did not depend solely on the presence or absence of deranged test results or observations, which were significantly present in both conveyed and non-conveyed groups. This provides a rationale for the difference in outcomes between the previous studies and the present evaluation, suggesting that the inclusion of telephone decision support from a senior clinician in addition to POCT had a significant impact on the actions and decision processes of the paramedic teams, and may have allowed for a more flexible and nuanced clinical approach, which increased the non-conveyance rate.
In the group of patients admitted to secondary care for further assessment, the high proportion of deranged blood results and observations and range of serious discharge diagnoses suggested a high prevalence of acute disease in this population. Comparing this with the low reattendance rate in the non-conveyed group suggests that this approach may have been effective in identifying patients with severe underlying illness.
A recent report based on prehospital assessment of elderly patients by a service in Dublin that included multidisciplinary assessment of patients with frailty syndromes suggested a far higher non-conveyance rate was achievable than that suggested by the findings of this evaluation (92% compared with approximately 75%). The lack of clinical detail in the report makes comparison difficult, but the included case report of a typical patient suggests a lower degree of clinical acuity than was present in this evaluation, which may explain the different findings between the two services (McNamara et al, 2020).
Limitations
This evaluation of a novel pilot service was based on a small convenience sample so the authors are unable to confidently extrapolate the results to the wider population.
The lack of an objective comparator means that the data are purely observational in nature. Longitudinal data on the patient group as a whole were limited to whether they were admitted to hospital over the next 30 days; for those who were not, there is limited clinical detail available about the nature of any subsequent community healthcare contacts, and the analysis is limited to information derived from hospital records.
The total number of patients visited and enrolled during this pilot project was low, despite the broad inclusion criteria; this is because few study-trained paramedic staff were available, as there was no funding to support dedicated paramedics for this project. As such, this project should be seen as a pilot proof-of-principle study and the results interpreted accordingly.
This service and study were made possible through the parallel mobilisation of a £63 000 winter pressures grant from the clinical commissioning group which was used in entirety to staff, modify and refit the rapid response vehicle (staffing £52,000, vehicle consumables and overheads £11,000), with the i-STAT machine and consumables provided free of charge from Abbott. This was a singular funding opportunity used specifically to trial this pilot study, and would be unlikely to be repeatable or scalable across other healthcare providers in the short term. Training was undertaken during shift time and was not directly funded.
The dedicated staffing was the key driver for the project's high cost. This approach was taken to allow the unit to focus specifically on calls where it would more likely to be of benefit. However, if the project was upscaled, costs could feasibly be mitigated by installing POCT devices in more vehicles or in potentially high-yield locations such as care homes, reducing the need for a dedicated unit.
The unit was also used to support wider service demands such as attending category 1 calls when it was not feasible or desirable to run the frailty response unit (e.g. when suitably skilled staff were not available).
Formal analysis of the cost-effectiveness of delivering this model as a full service was not undertaken, but the significant reduction in conveyance seen in this evaluation offers a potential for marked cost savings in terms of hospital admissions.
The telephone decision support service, while long established as a 24-hour standard service for all medical referrals in Oxford and theoretically feasible in most hospitals, is not yet available in all trusts in the UK, which could limit the implementation of this service across the wider NHS in the short term.
At the time this work was undertaken, there was no easily portable, reliable POCT available for inflammatory markers such as C-reactive protein, which would have been useful at this clinical decision point, and commonly requested blood tests such as liver function and full blood count were also not available at the point of care.
The i-STAT platform takes approximately 10 minutes to process results per cartridge, which could potentially lengthen on-scene times for paramedics, although these tests can be run in parallel with other clinical assessments, which would improve efficiency. The effect of including testing on on-scene times was not covered in this study.
Furthermore, the potential benefit of bedside imaging such as point-of-care ultrasound was not explored, nor was use of video streaming to facilitate clinical assessment.
The impact of including the use of ancillary services such as hospital-at-home was beyond the scope of the project. Incorporating these into future studies may yield a more comprehensive assessment of community-based acute medical care in this population.
Implications for practice
This integrated assessment service as outlined in this evaluation involves an extension of secondary care expertise and resources to clinical areas outside the traditional confines of the hospital, while simultaneously using the hospital's clinical expertise, information technology and governance processes through the telephone advice and decision support.
These resources may enhance the situational capabilities of specialist paramedics, offering a more nuanced and flexible approach to the management of frail elderly patients in the community.
Extending the range of diagnostics (especially the measurement of inflammatory markers such as C-reactive protein) could expand these capabilities and potentially guide the effective administration of therapies such as antibiotics and diuretics.
Liaison with community frailty services such as physiotherapy, occupational therapy and social work delivered through models of care su ch as hospital-at-home offers the potential for the coordination of packages of multidisciplinary care across repeated visits and could, ultimately, further reduce reliance on hospital admission to deliver acute healthcare to this vulnerable population.
Conclusion
The results from this study suggest it is feasible to perform POCT as part of clinical assessment offered by ambulance services, and that, by offering access to secondary care resources (diagnostics and clinical assessment) in a community setting, a proportion of older patients could potentially be managed in a home setting without physically attending secondary care and without adding significantly to the burden on community services.
POCT combined with telephone decision support may be effective in facilitating alternatives to hospital admission for frail patients in supportive care environments. Larger scale, systematic evaluations are warranted to fully establish utility and cost-effectiveness.