
You arrive on scene and, following a safety <C>ABCDE assessment, discover a 30-year-old conscious trauma victim who has suffered blunt trauma to the chest in a fall from a standing height onto a concrete bollard. Blood pressure is 140/84 mmHg; pulse is 96 beats per minute; and respiratory rate is 20 breaths per minute. The trachea is central and there is decreased chest movement and air entry on the side of the injury over an area of extreme tenderness. Oxygen saturations on air are 94%. Does this patient require needle decompression of their chest?
Needle decompression of the chest
Needle decompression of the chest (also known as thoracocentesis or thoracentesis) is a manoeuvre to release abnormal air from the pleural space. Prehospital needle decompression is only indicated for patients suffering from tension pneumothorax; this is an accumulation of air under tension that displaces the mediastinum, causes diaphragmatic depression (and inversion), impaired venous return and respiratory compromise—and ultimately cardiac arrest. This is different from a simple pneumothorax where the air merely occupies the pleural space and there are no pressure effects. Tension pneumothorax is an uncommon event in UK civilian major trauma patients, and especially uncommon in the self-ventilating patient (Leigh-Smith and Harris, 2005).
A recent European study showed that paramedic-performed prehospital needle decompression of the chest was carried out in 0.7% (17/2261) of adult trauma patients admitted to a level 1 trauma centre over 6 years (Kaserer et al, 2017). When looking exclusively at blunt trauma, as is common in the UK, a Canadian series over 3 years found the rate of needle decompression to be 1.4% of level 1 trauma patients (Ball et al, 2010). Current rates of needle decompression for trauma patients are similar to rates from 20 years ago: around 1–2% (Eckstein and Suyehara, 1998; Cullinane et al, 2001). It is acknowledged that rates of needle decompression are substantially higher in patients evacuated by helicopter rather than by ground (Cameron et al, 1993; Eckstein and Suyehara, 1998). The low frequency with which prehospital needle decompression of the chest is performed may justifiably engender a lack of confidence among paramedics faced with real-world patients. When one considers that only one in five hundred (0.2%) paramedic advanced life support attendances (of all causes including medical) result in a needle decompression (Warner et al, 2008), the rarity of this particular intervention for the typical paramedic is dramatically underlined.
The aim of the current article is to present a small case series of inappropriate needle decompressions from a single UK major trauma centre, and to encourage UK prehospital care providers to think carefully about needle decompression in chest trauma patients.
Case reviews
Case reviews from a mixed urban and rural major trauma centre (MTC) have revealed a number of needle decompressions performed in the prehospital setting that were unwarranted. Indications appear to have been based around clinical signs; namely decreased chest movement and decreased breath sounds. Some have reported an apparent hiss of air after removing the needle from the cannula.
Specific images
To illustrate the unwarranted nature of some of the needle decompressions, three computed tomography (CT) scan images from three different patients have been selected (Figures 1–3). The CT scans were performed in the MTC emergency department (ED) after the primary survey, and within minutes of reception as is customary in the receiving trauma centre.
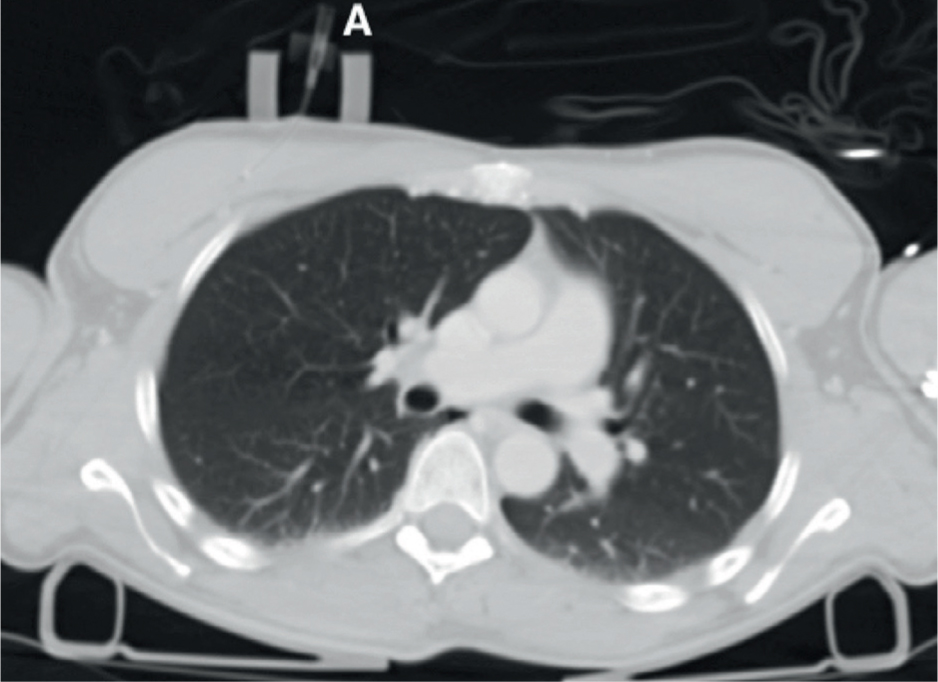
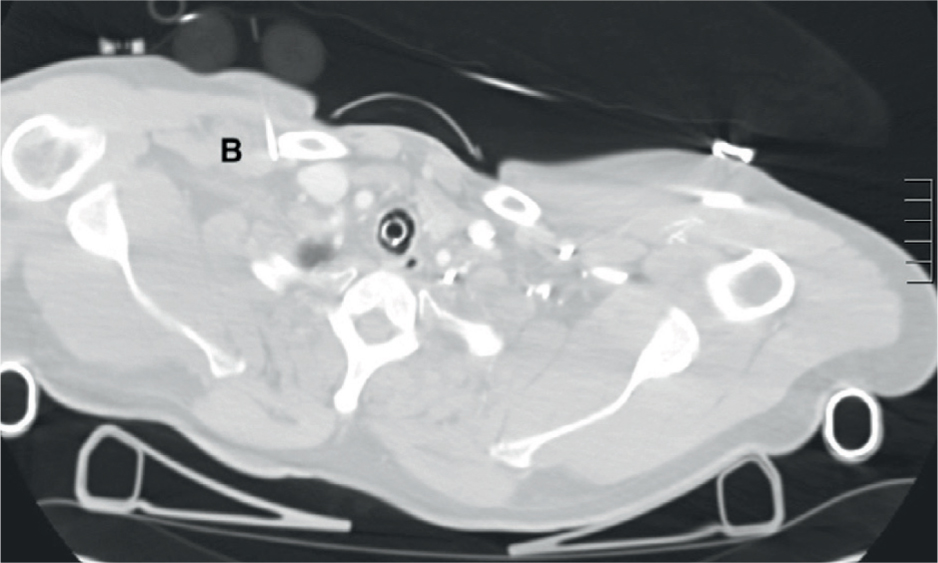
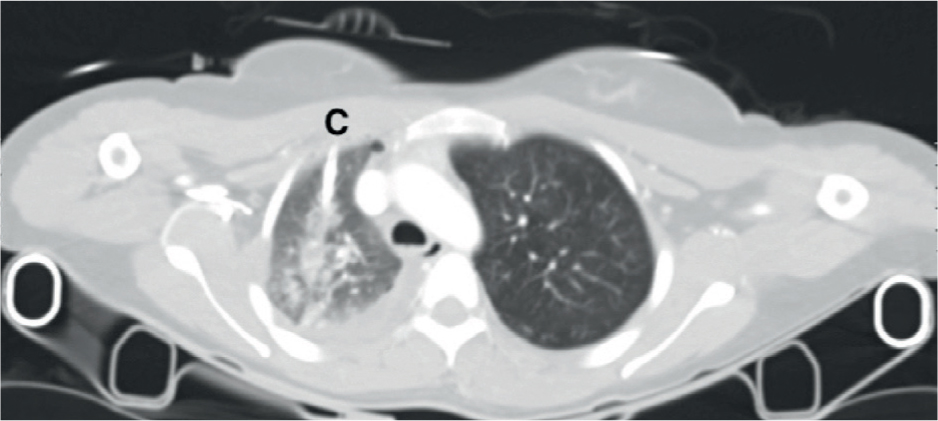
None of the patients had a clinically significant pneumothorax on CT scanning after arrival in the ED and none subsequently developed tension pneumothorax. Given that the CT scan may be performed some time after needle decompression (up to 60 minutes), one might suppose that a prehospital tension had been successfully treated. This might be the case; however, needle decompression would not be expected to completely resolve signs on a CT scan, and there would likely be evidence of a residual pneumothorax. There is no evidence of residual pneumothorax on any of the images shown (Figures 1–3), suggesting that the prehospital needle decompression was unwarranted. In the authors' opinion, although this method cannot be truly certain of ruling out a prehospital pneumothorax, it is a fair assumption, and one that has been applied in recent studies (Kaserer et al, 2017).
What is responsible for the patient's physical signs?
It has been demonstrated that needle decompression was not indicated for the three cases shown in Figures 1–3. Despite this, the prehospital care providers were sufficiently worried about their patient to perform an intervention. The current article seeks to better explain the clinical signs that suggest life-threatening tension pneumothorax, and encourage paramedics to think critically about alternative chest pathology before performing needle chest decompression. Unilateral decreased air entry with decreased movement of the chest may be caused by a number of factors other than tension pneumothorax, namely:
It is important that these factors are considered alongside the possibility of a tension pneumothorax within the context of an appropriate chest examination. The Joint Royal Colleges Ambulance Liaison Committee (JRCALC) guidelines 2016 suggest a Feel, Look, Auscultate, and Percuss approach concentrating on breathing adequacy, respiratory rate, volume, and equality of air entry (JRCALC and Association of Ambulance Chief Executives (AACE), 2016).

Tension pneumothorax in different modes of ventilation
In the authors' opinion, paramedics should be relatively reassured if their patient is breathing unassisted, and substantially more worried about tension pneumothorax leading to cardiac arrest if their patient is requiring assisted ventilation. This is because patients with tension pneumothorax who require assisted ventilation are 17 times more likely to progress to cardiac arrest than those with a tension pneumothorax who are breathing unassisted (Roberts et al, 2015).
In patients receiving positive pressure ventilation (bag-valve-mask or ventilation via a supraglottic airway or endotracheal tube), the onset of a tension pneumothorax can be rapid; as such, patients usually present at the point of decompensation (Leigh-Smith et al, 2012). Suspicion of tension pneumothorax in these patients should therefore be heightened. The classically taught signs include:
It is important to realise that these clinical signs are not always present; indeed, the only reliable signs that are always present are tachycardia and respiratory distress (Leigh-Smith and Davies, 2003).
End-tidal carbon dioxide (ETCO2) may be deranged in tension pneumothorax. Initially, ETCO2 increases as ventilation is compromised and carbon dioxide builds up in the lung. Once the mediastinum is compressed, perfusion is impaired and less carbon dioxide is delivered to the lung causing ETCO2 to fall (Sullivan, 2016).
If clinical signs are suspicious for tension pneumothorax, after having checked the airway, the chest should be decompressed. This may be via needle decompression or by open thoracostomy; enhanced care teams may consider open thoracostomy in patients ventilated with positive pressure suspected of having a tension pneumothorax. Ultrasound may be used to augment the diagnosis. Enhanced care teams may also perform bilateral thoracostomies in the event of traumatic cardiac arrest as they try to quickly rule out reversible life-threatening causes.
Special note should be made of the following circumstance that may trap the unwary paramedic. When one side of the chest has a haemothorax, the uninjured side opposite will appear more resonant. This may be mistaken for hyperresonance (but is actually a result of decreased resonance in the injured side) and needle decompression may be attempted in the uninjured side. Bruising, pain, crepitus, and decreased chest wall movement may be evident on the injured side, and if you find yourself performing a needle decompression on the opposite side to such obvious injuries—take a moment to confirm your suspicions.
What are the most appropriate actions for the clinical vignette?
Unless there is a history of chronic obstructive pulmonary disease (COPD), give oxygen to restore a normal SpO2 (98%), administer effective analgesia and frequently reassess the patient. This patient will not require prehospital needle decompression. If there is a history of COPD, aim for SpO2 of 88–92%.
Does unnecessary needle thoracostomy cause any harm?
If you have carried out needle thoracostomy when it is not necessary, you may have produced a minor pneumothorax (which usually reabsorbs). However, during transfer, the patient should be regularly reassessed for any change in chest symptoms or signs as there is a small risk that any pneumothorax could progress. There is a potential risk of damage to underlying structures such as the lung itself, or blood vessels of the chest. There is also a slight risk of developing infection in the pleural space, lung, or chest wall as a long-term complication as these procedures are often undertaken without strict aseptic precautions (Leigh-Smith and Harris, 2005).
Correct actions regarding possible tension pneumothorax
To justify needle decompression, the patient should be frequently reassessed for the following deteriorating respiratory signs:
If the patient is in extremis (and you assess cardiac arrest to be imminent), proceed immediately to needle decompression.
The authors would like to repeat the Advanced Trauma Life Support (ATLS) message that needle decompression is appropriate for patients in a critical condition with rapid deterioration who have a life-threatening tension pneumothorax (American College of Surgeons (ACS), 2012). The National Institute for Health and Care Excellence (NICE) (2016) guideline [NG 39] advises to only perform chest decompression if there is haemodynamic instability or severe respiratory compromise. Paramedics should be reminded that there are other causes of decreased air entry and chest movement besides tension pneumothorax.
The current article is written for the paramedic practising within the UK civilian trauma network, with the majority of patients suffering blunt trauma. Tension pneumothorax is more common with penetrating trauma, particularly due the ‘one-way valve’ that may be created by injured soft tissues, the so-called ‘sucking chest wound’. The clinical signs of tension pneumothorax will remain the same whether as a result of blunt or penetrating trauma, but clinical suspicion should remain higher with penetrating chest injuries.