
The fascia iliaca compartment block (FICB) aims to provide anaesthesia and analgesia to the anterior compartment of the thigh, thereby providing analgesia for fractures to the femur and neck of femur, as well as potentially for soft-tissue injures to this area.
It does this by interrupting the conduction of nerve impulses by the femoral nerve and lateral cutaneous nerve of the thigh. An FICB does not provide analgesia or anaesthesia to the distal leg below the knee, which is supplied by the sciatic nerve, nor to the medial aspect of the thigh, which is supplied by the obturator nerve.
A short guide is presented to the landmark approach to FICB, and the choice of local anaesthetic volume to be given by patient's estimated weight.
The technique
FICB is a simple technique, and allows a high quality of analgesia to be given without the side effects of opiate analgesia. FICB is the current gold standard in the management of neck of femur fractures with pain unresponsive to intravenous opioids and paracetamol (National Institute for Health and Care Excellence (NICE), 2017). It is frequently performed in emergency departments, but has also been used as a prehospital intervention by nurses and paramedics, where it has been demonstrated to be both safe and effective (Hards et al, 2018), without reducing on-scene times (McRae et al, 2015).
The technique is easy to learn and can be undertaken using a landmark technique or with ultrasound guidance (Chesters, et al, 2009). A sample technique monograph is included in Table 1. Although point of care ultrasound (PoCUS) is becoming more commonplace in prehospital care and paramedic practice across the country, it is unlikely that PoCUS will be available on all frontline ambulances in the near future. Therefore, this article will focus on the landmark technique, which is still widely used. Use of FICB has been shown to be associated with a reduced need for opiate analgesia and is likely to lead to more effective pain relief, with fewer side effects, than oral or injected analgesics (Fadhlillah and Chan, 2017; Kassam et al, 2018). FICB is also likely to lead to improved patient outcomes (Callear and Shah, 2016), including increasing a person's chances of returning home on discharge from hospital (Bray and Collins, 2015).
| Fascia iliaca compartment block | ||
|---|---|---|
|
Indications
|
Side effects
|
|
|
Contraindications
|
||
|
Administration
|
||
|
Weight
|
Volume (of 0.25% solution)
|
|
Landmark technique
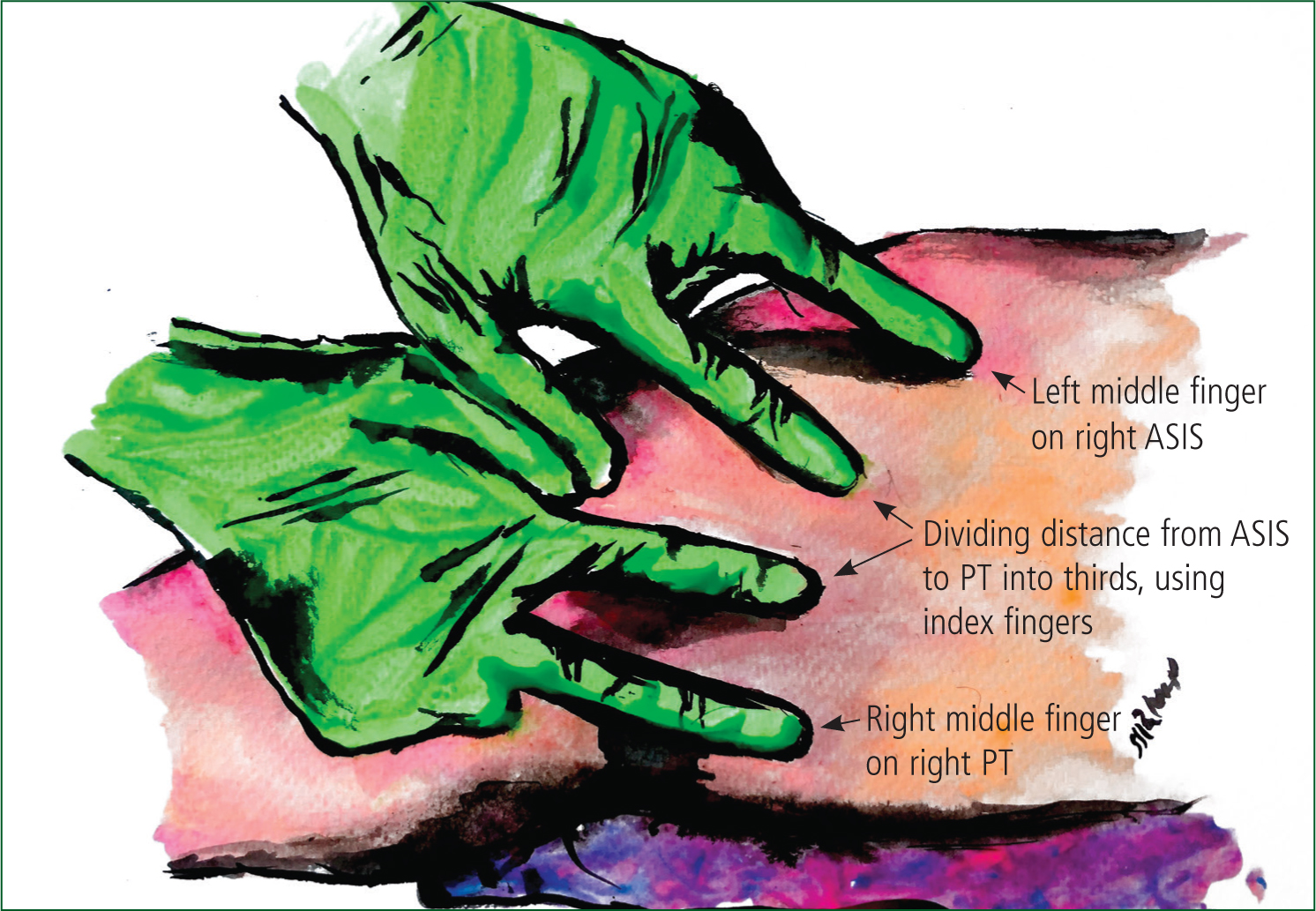
The location for FICB must be correctly identified to minimise risk of complications. The first two important landmarks are the anterior superior iliac spine (ASIS) and the pubic tubercle of the pelvis. These two points are connected subcutaneously by the inguinal ligament, the next important landmark. The length of the inguinal ligament needs to be divided into thirds; this can be easily estimated using the index and middle fingers of each hand. From this point, the site for injection is located 1–2 cm distally from the junction of the lateral and middle third. The femoral artery can be palpated medially to the puncture site prior to undertaking the technique to reassure the practitioner that their chosen site is distant from the large neuromuscular bundle in the thigh (Figure 1).
The point for injection can be marked with pressure from the blunt end of a needle or a needle cover before a sterile area has been created. The area surrounding the injection site is then cleaned with 70% isopropyl alcohol or chlorhexidine and allowed to dry (this is especially important when chlorhexidine is used, as it is a potent neurotoxin). The skin can now be anaesthetised with around 2 ml of 1% lidocaine if required.
A short bevelled or blunted needle attached to the syringe holding the levobupivicaine is now inserted through the skin at a 90o angle. The needle is advanced, producing two palpable ‘pops’ as the needle perforates the fascia lata and the fascia iliaca. After advancing another 1–2 mm, aspiration is attempted to verify that the tip of the needle is not within a blood vessel. Once negative aspiration has been observed, injection can begin. While the procedure may feel uncomfortable, there should be little resistance and the patient should not experience pain on injection. Once the volume desired has been injected, remove the needle and dispose of this safely, then apply gentle pressure to the area for around 2 minutes. Analgesia will become apparent over the next 10–30 minutes; during this time, vital signs should be monitored and the patient observed for signs of local anaesthetic toxicity (Box 1).
Conclusion
FICB is a safe and effective means of providing analgesia for injuries to the anterolateral thigh or femur, and although not currently a technique widely used by paramedics within the UK, it is certainly on the horizon for specialist and advanced paramedics nationwide. A short guide to the technique has been presented here for education and reference, although this does not replace comprehensive teaching and supervised practice to achieve clinical competence.