
In order to meet the requirements for safer manual handling, with equipment such as tail lifts and ramps, dual-crewed ambulances (DCAs) are typically increasing in weight. This has resulted in reduced fuel economy, higher running costs and poorer driving characteristics. Additionally, the NHS has identified the need for a more integrated clinical model (Department of Health and Social Care (DHSC), 2011) providing more ‘see and treat’ services instead of transporting patients to emergency departments (EDs). These two factors suggest that both evolved and entirely new types of emergency vehicles will be needed to meet future requirements of ambulance services.
This pilot project aimed to investigate the potential of smaller, lighter, rapid response vehicles (RRVs) in order to:
Vehicle environmental context
The NHS accounts for 5% of all road traffic in England, with staff, patients and visitors travelling over 20 billion kilometres annually by car (GrEAN, 2011). The Climate Change Act [2008] has committed the government to low carbon transport and ambulance fleets have already considered low carbon solutions including an Eco Driving initiative, estimated to save £1.5 million per annum (GrEAN, 2011). Prior research at Loughborough University considered the role of electric vehicles and highlighted the potential of solo response vehicles to reduce carbon emissions (Hignett et al, 2012a).
Vehicle performance context
Changes in UK government policy encourage a shift away from emergency care and towards urgent pre-hospital care. This means providing assessment, diagnosis and treatment for patients in their own homes or at the call site; as such, these changes are increasing the number of solo responders with enhanced clinical skills (DHSC, 2006).
Following the introduction of ambulance quality indicators, ambulance services in England have been required to send an emergency response, with a defibrillator, within 8 minutes to 75% of Category A (Red 1) emergency calls (North East Ambulance Service (NEAS), 2017). Unfortunately, this standard has been frequently missed since its introduction in 2011 (National Audit Office (NAO), 2017).
After the emergency response had reached the scene, for over 50% of calls a dispatched ambulance was not required and the patient could have been referred to alternative medical treatment (BBC News, 2014). About 40% of the 10.3 million visits to EDs in England in 2009/10 ended with the patient only needing advice and no specific treatment (NHS Digital, 2010). It is reported that, in some cases such as heart attack and stroke, some patients have better outcomes by going straight to specialist centres. However, for other patients, being seen in a primary or community care setting (i.e. not sent to EDs) would provide more appropriate care and a better patient experience (NHS England, 2013). This approach was explored by the CURE project at Loughborough University, which demonstrated how non-critical, pre-hospital care could be delivered using portable pods/packs and mobile treatment units (Hignett et al, 2012b).
Other modes of transport have been trialled and found to be as effective as RRVs, e.g. motorcycles in Scandinavia have been shown to respond on average 1 minute faster in cities (Nakstad et al, 2009). In the UK, the use of motorcycles is limited and numbers have been reduced owing to concerns about rider safety with respect to weather conditions and night working. However, a recent Australian trial has illustrated their usefulness in providing ‘shorter response times for urgent cases and freed up road ambulances’ (EMS1, 2015).
In 2015, the Association of Ambulance Chief Executives (AACE) set out its vision of ambulance services for 2020, where the ambulance becomes a connected mobile treatment centre. This includes advanced clinicians who are trained and supported to manage more patients at home so that the ambulance sector becomes both a ‘coordinator of clinical and social responses and a mobile healthcare provider, operating in a range of settings’ (AACE, 2015).
Phase 1: Stakeholder consultation
Method
Five stakeholder consultations of approximately 45 minutes were undertaken with two ambulance Trust fleet managers, the technical manager of a vehicle converter (ambulance manufacturer), a paramedic with over 10 years of experience and the head of the Ultra-Light Vehicle Research Group to gain an understanding of current, short- and medium-term requirements with respect to:
The semi-structured interview data were recorded and analysed qualitatively using a thematic approach resulting in six themes:
Results
Vehicles used
The majority of vehicles used by the two fleets were DCAs. Trust A had approximately 300 van conversion DCAs and Trust B had approximately 140 cab (box) conversions. Trust A expressed a preference for lowering the suspension (low floor kneeling) and ramp access to the ambulance because it was felt to be more reliable than the tail lift option. However, both trusts reported that DCAs were not generally considered to have good handling characteristics.
Operationally, it was reported that the first response was usually with an RRV and followed by a DCA. The trusts reported that 4x4 RRVs were preferred because of better driving characteristics in a range of conditions. Motorbike paramedics had not been used by the trusts for a number of years because of concerns of rider safety, high vehicle running costs, and limited operational conditions.
Responder working day
The responder working day was reported to be varied, including driving to standby points and waiting for the next call, with DCA staff sometimes waiting in the back of the vehicle between calls so that they are not visible to the public. As well as many calls being stood down, significant waiting at EDs between calls and very full, busy shifts were reported. Therefore, maintaining the comfort and confidence of staff was felt to be key, including having the right kit, comfortable vehicle seating, heating and cooling—factors that can be influenced by both vehicle specification and manufacturer. Increasing difficulties in recruiting RRV staff were reported owing to a reluctance to lone working.
Patient outcomes
The stakeholders reported that most calls do not necessarily require transporting but that patients are increasingly requesting to go to hospital as this is seen as the most risk-averse option and they believe that this will give a better outcome. It was felt that patients were not generally aware of the differing types of emergency response and expected to receive an ambulance to a call.
Future of service
Call response time targets were not felt to be a good measure of performance. The stakeholders expressed their opinion that future targets should also include a measure of patient outcomes. They felt that in the long term, this would be more likely to encourage the ‘at-home’ service options, which in turn would influence changes in vehicle types.
Reducing carbon emissions
The two trusts reported that their fuel bills were approximately £6 million per annum. It was discussed that targeting the right resources for the right jobs was a key method in reducing these costs, as well as not leaving vehicles on standby or being stood down, e.g. part way through a response. Alternative fuel vehicles, such as electric, were not seen as a workable solution in the short to medium term because of real-world performance and operational compromises.
Ideal future vehicles
New technologies and processes are creating lightweight vehicles across the automotive industry that are becoming available for ambulance conversions. It was felt that there was the potential for the ambulance cab conversions to move toward a complete composite construction to reduce overall weight. In particular, there is an opportunity to consider specific design challenges such as creating a lightweight composite tail lift or ramp to reduce weight and improve driving characteristics.
It was also felt that there is an opportunity for smaller RRV vehicles, particularly within city centres but only in small numbers, while DCA ambulances would continue to provide the majority of responses.
Phase 2: Concept generation and evaluation
The data from the first phase were used to explore the new vehicle market potential by focusing on the apparent gaps and opportunities to provide:
These two opportunities were used to generate design concepts. Concept A for an agile fast response vehicle (cost range £16 000–£35 000) as an option between motorcycles and RRVs, and Concept B for a versatile RRV (cost range £35 000–£110 000) as an option between RRV and DCAs.
Concept A: Agile fast response vehicle
Concept A proposed a smaller, lighter, agile fast response vehicle (FRV) (Figure 1) to reach the patient quickly, particularly in congested urban areas or where access for a DCA would be difficult. This aimed to address duplication of resources where both an RRV and DCA were dispatched—with one being stood down during the response. For the future integrated care model with more patients treated at the scene, the agile FRV could provide a resource-efficient method to reach patients. The vehicle would be single occupancy, fully enclosed, crash worthy and with good load-carrying capacity while retaining the agility of a motorcycle.

Concept B: Versatile RRV
This concept offered support for the future integrated service provision with a smaller vehicle than the DCA to replace current RRVs and support more options for treatment at scene. The design included the visibility of a DCA but with car-like driving characteristics. If the vehicle was dual-staffed, it could also be fitted for patient transport which might be particularly suitable for more mobile patients and those not requiring ED transportation. A key feature of the rear-access vehicle (Figure 2) was the lowering floor to give easy-level access and clearance to work while standing when the vehicle is stationary.

The side-access option (Figure 3) proposed a more cost-effective design by using a rotating patient chair. It was proposed that this could require minimal vehicle modifications while still providing treatment capabilities within the vehicle.

Evaluation and responses
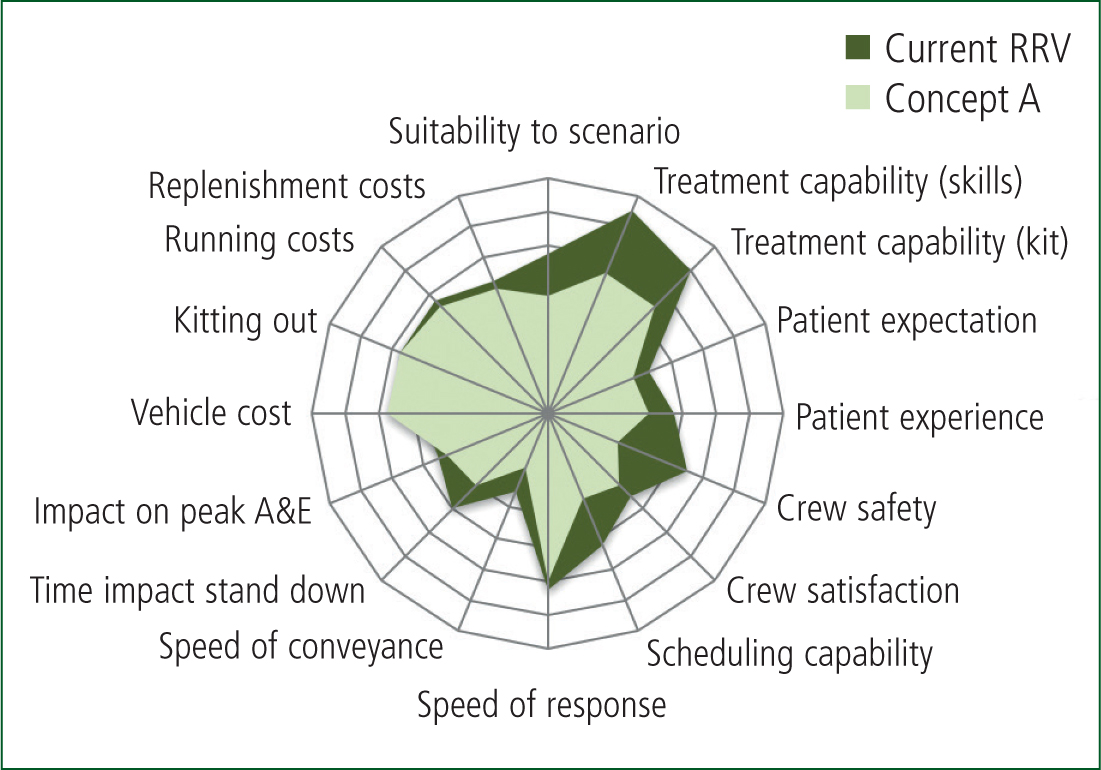
Evaluation of the concepts was invited using an online questionnaire with responses received from four NHS trusts across the UK, a total of 8 fleet managers and clinicians. Two applicable patient scenarios (Table 1) developed by Hignett et al (2012b) were used to present the concepts and an adaptation of the traffic light model (Royal College of Art, 2010) was used to specify and score features using a five-point Likert scale, enabling a comparison of the concepts with existing DCAs and RRVs for a scenario.
| Scenario 1 (RRV and Concept A comparison) | Scenario 2 (DCA and Concept B comparison) | |
|---|---|---|
| Patient | Male, late 40s, known chronic respiratory condition, chest pain | Female, elderly 70+ years |
| Symptoms | Shortness of breath on exertion | Open wound above left eyebrow, significant bleeding has stopped, some headache, minor level of disorientation |
| History | Long term chronic obstructive pulmonary disorder (COPD), deterioration over 2 weeks | Mechanical fall, remembers tripping over, hit head but nothing specific, just ended up on the floor |
| Expected ECP action | Full patient assessment, ECG and respiratory assessment, nebulisers with oxygen therapy | Full patient assessment; blood pressure, temp, blood sugar monitoring, to establish reason for fall. Two stitches above eye |
| Environment | Town centre, shopping district at evening rush hour | Rural village midday |
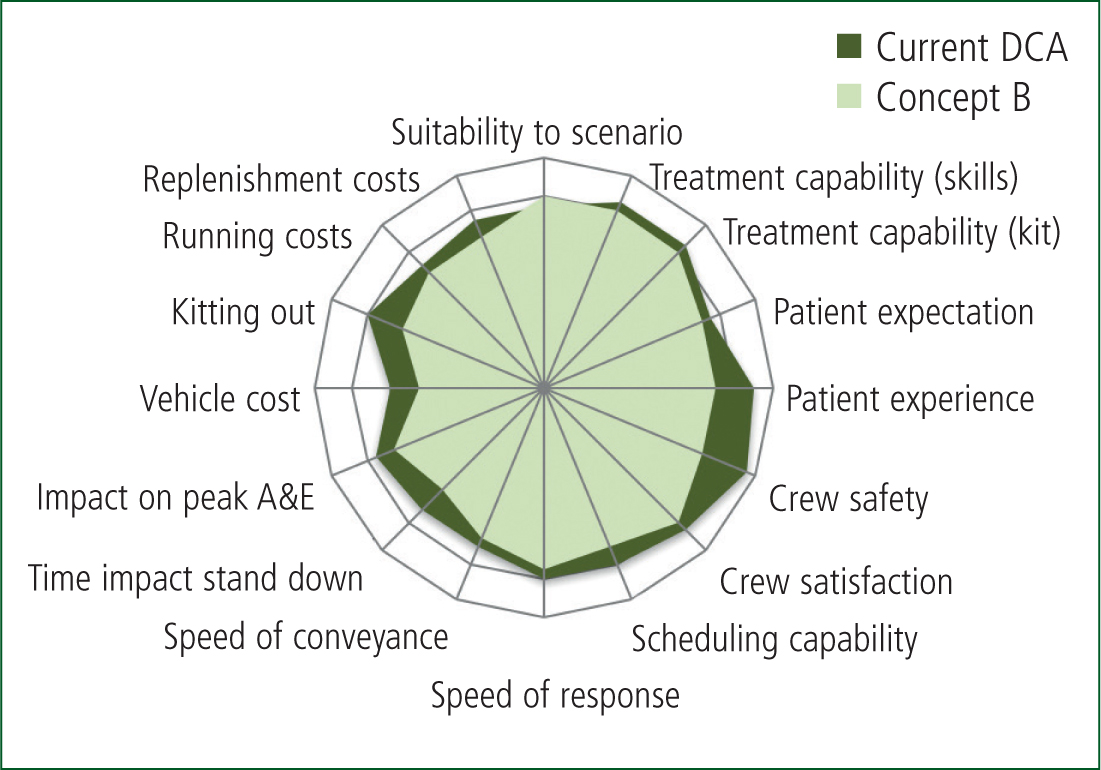
The results of this vehicle feature comparison can be seen in Figure 4 and Figure 5, the larger plot sizes illustrating higher respondent rating of feature suitability. Additional data were collected with telephone interviews to expand the responses where appropriate.
Changes in fleet provision
Three of the four trusts had increased the number of DCAs over the past 15 years and envisioned that this trend would continue while RRV numbers were likely to decrease or remain the same.
‘…the only resource we have added over the past 15/20 years are FRVs and this is only because they are faster and can hit the Category A calls quicker. I can't see things changing much over the next 15 years; we need more DCAs to transport patients. We have tried educating the public not to call 999 but that has not worked.’ Respondent 5 (Clinician)
Reducing carbon emissions
Respondents were asked to prioritise where they felt the greatest impact for reducing carbon emissions in the next 15 years could be achieved. Their ranked order list was:
Additional interview details highlighted the impact on fuel consumption for vehicles left running on standby and on run-lock—where the vehicle is locked but left running to provide ancillary power. One trust reported that almost 20% of vehicle running time was on run-lock which did not include standby running with the crew inside the vehicle. This is perhaps an area where ‘stop-start’ technology has significant potential to improve functionality and fuel economy.
Future service provision
Ambulances will require improved patient assessment capacity to meet ‘see and treat’ service demands and will need to carry more sophisticated diagnostic and communication aids.
‘More ‘see and treat’ such as your small van concept with enhanced clinical skills for paramedics.’
Respondent 8 (Clinician)
Concept feedback
Concept A: Agile RRV
Half of the respondents felt that Concept A could be a useful addition to the fleet, but there were concerns about vehicle safety and crew satisfaction. However, the vehicle could provide a fast, cost-effective response particularly in urban and congested areas.
‘(Useful for) city centre work; busy events over large areas.’ Respondent 7 (Clinician)
Concept B: Versatile RRV
Concept B was also felt to offer some design options as a useful addition to the fleet. Concerns were raised by fleet managers that the cost outlay of the new design might not provide significant advantages over a DCA van conversion and that there may be reliability issues with the lowering floor. Clinicians were generally more positive about Concept B over Concept A.
‘(Useful for) any RRV scenario, good opportunity to get patients out of the public eye. Very worthwhile and better than traditional RRV.’
Respondent 5 (Clinician)
The side-access option for Concept B was felt to be useful for getting patients into a vehicle but there were concerns that if a patient required treatment laying down, this could be complex and that clinical infection control could be harder to manage in the smaller space provided.
Concept C: Superlight DCA
During the evaluation phase, it emerged that in the short/medium term, a superlight DCA (Concept C) could provide the greatest benefit and allow for flexibility in service provision. Reducing vehicle weight could be best addressed through cost-focused design innovation (Niche Vehicle Network, 2015). For the van conversion, composites to address weight issues such as tail lifts and equipment storage through an integrated vehicle structure could be used.
Conclusion
The current feasibility study indicates that policy change to support the integrated clinician service model could create a future market for smaller, lighter vehicles. The study indicates that the most pressing issue is to improve fuel economy in the immediate future and this would probably be best achieved through increased fuel economy via the adoption of technological solutions for existing DCAs.
Three new vehicle types have been identified to inform further research. There is a small potential market for an agile single crew FRV particularly in urban areas. This type of vehicle could be based on an adaptation of a three-wheeled leaning scooter, but would require development of passive safety and car-like crash testing to demonstrate suitability. The demand for these vehicles is estimated to be up to 20 vehicles per trust.
There is a small initial market, up to 100 vehicles per trust, for a versatile RRV that is likely to increase as the ambulance service moves toward an integrated service provision with more ‘see and treat’ cases
However, the feasibility study indicated that the superlight DCA might have the greatest market potential in the short to medium term—up to 500 vehicles per trust. As cities require ultra-low emission vehicles and if a comparable cost can be achieved, there are opportunities to minimise the weight of DCAs using composites, e.g. monocoque for the vehicle structure, internal and external panels, to reduce carbon emissions and improve driving performance.
Further work across all UK trusts should be carried out to enable a more detailed picture of future vehicle demand. Additionally, a study specifically designed to research patient perceptions of not using DCA vehicles, when clinically appropriate to a scenario, will help to understand the role of vehicles in supporting an integrated clinician service model to enable ‘care as close to home as possible’ (House of Commons, 2017).