Meningitis and septicaemia strike without warning and can kill in hours. Few infectious diseases have such a devastating impact. The disease can bring a healthy person near death within 24 hours. Babies, children and young adults are most at risk from meningitis and septicaemia, and as many as one in ten people who get the disease will die (Prasad and Karlupia, 2007).
Of those that do survive, one quarter will suffer from long-term effects such as deafness and epilepsy. While several vaccines, including the highly successful MenC, have had a huge impact on disease incidence, lack of a universal vaccine that protects against all forms of the disease means that recognizing the signs and symptoms is key to combating this deadly disease.
In particular, knowledge of the recently identified early warning ‘red flag’ symptoms can help speed up diagnosis and treatment and help to improve outcomes.
Meningitis Research Foundation
The Meningitis Research Foundation (MRF) provides resources for health professionals to help diagnose and treat meningitis and septicaemia. Recently, MRF re-launched its life-saving series of algorithms for the management of meningococcal disease and bacterial meningitis in children and young people. These protocols are aimed at doctors in emergency medicine, paediatrics, paediatric intensive care units, anaesthetics and general medicine in the UK.
Resources for paramedics
Often, ambulance personnel are the first port of call for a seriously ill patient and will be responsible for managing them while transporting them to hospital. As a result, MRF has also developed a resource for ambulance personnel to facilitate early recognition, prompt treatment and appropriate management of patients with meningococcal septicaemia, in collaboration with the Joint Royal Colleges Ambulance Liaison Committee (JRCALC).
‘The disease can bring a healthy person near death within 24 hours’
To enable effective implementation of the benzylpenicillin mandate and achieve a better outcome for patients affected, the resource gives ambulance personnel practical, accessible information to help them identify and manage this life-threatening disease as early and effectively as possible.
Clinical presentations
There are two main clinical presentations of meningitis and septicaemia. These can occur on their own but often appear together. Septicaemia in the absence of signs of meningitis can be even more life-threatening than meningitis alone.
Meningococcal septicaemia occurs when meningococcal bacteria invade the bloodstream and release their toxic products. This can progress rapidly to shock and circulatory collapse. Deterioration can be rapid and irreversible, with treatment becoming less effective by the minute. The speed with which the disease is identified and treatment started mainly determines the outcome.
The ‘red flag’ symptoms: improving early recognition of meningitis and septicaemia
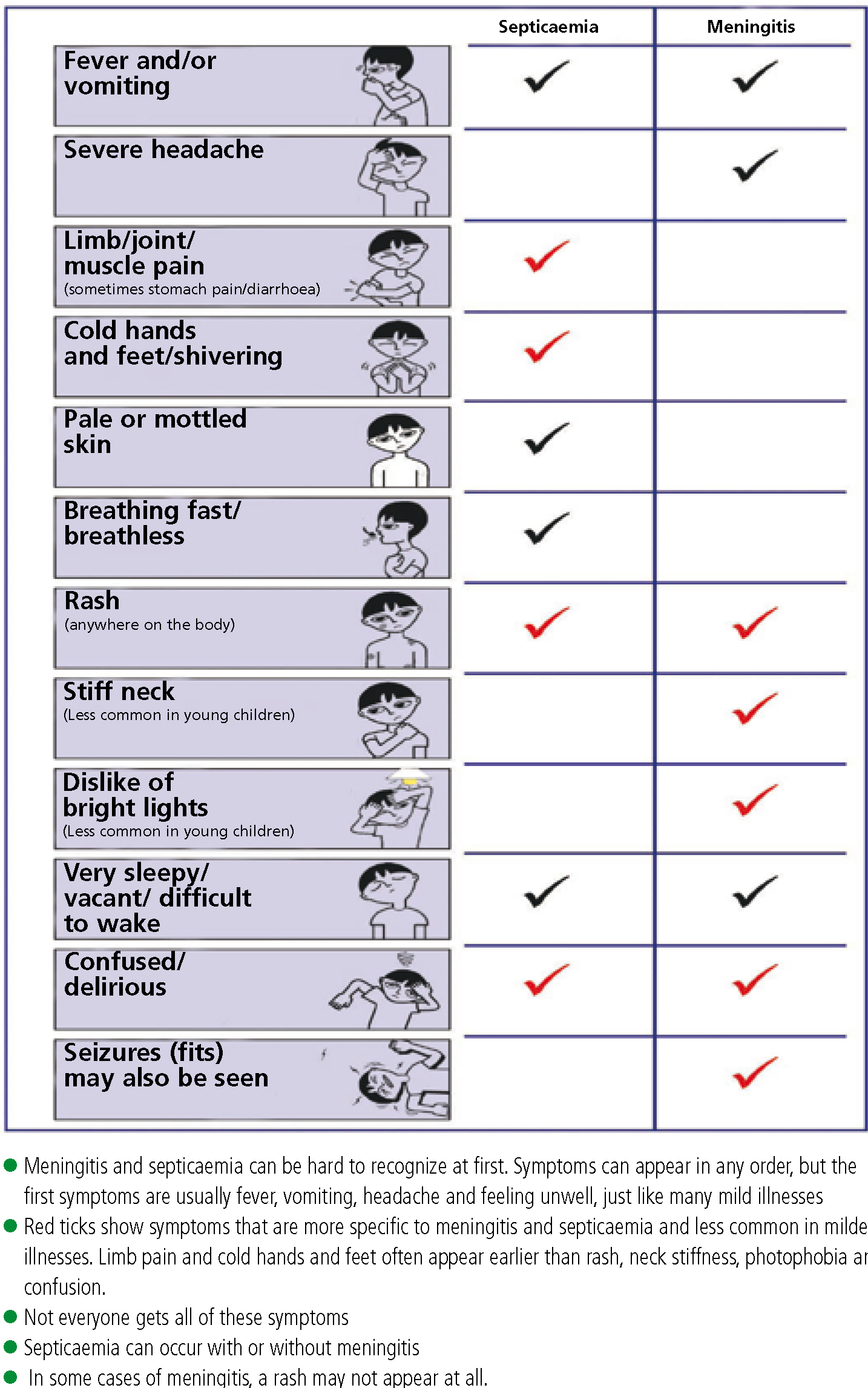
Although rapid identification and treatment of this disease provides the best chance of recovery, it can be very difficult to recognize. Symptoms can appear in any order, but the first symptoms are usually fever, vomiting, headache and feeling unwell; similar to many mild illnesses.
Recently published research funded by MRF (Thompson and Ninis, 2006), aimed to find out whether there were common early symptoms of meningitis and septicaemia, which if recognized at an early stage, could save lives. This was the largest study of its kind, and unique in investigating how children and adolescents with meningococcal disease present in primary care, and instrumental in building guidelines for diagnosis and identifying children at risk. The study found subtle ‘red flag’ symptoms that can be detected during the early stages (Figure 2).
Pale mottled skin is also a common feature of viral illnesses, but subsequent research found that limb pain and cold hands and feet help to distinguish patients with meningococcal disease (Haj-Hassan et al, 2011).
The rash
Any patient with fever and flu-like symptoms should be assessed regularly for the appearance of a non-blanching rash. However, in some cases, there may be no rash or it may appear late. So do not only look out for a rash. Also, up to 30% of cases start with a blanching pink rash which later becomes purpuric (Figure 1).

Conclusion
Time is critical with this disease and evidence has shown that early treatment with benzylpenicillin can reduce deaths from meningococcal infection. In 2000, paramedics in Scotland, Wales and England became the first in the world to give benzylpenicillin to patients with suspected meningococcal septicaemia.
MRF's ambulance personnel information has been updated in line with the latest JRCALC guidelines. It is available in two formats:
Anyone requiring further copies can obtain them, and other Foundation resources, free of charge by using the online ordering service (MRF, 2011). Please visit: http://tinyurl.com/437o746.