
Search and Rescue (SAR) helicopter paramedic winchmen are part of a four person crew manning SAR helicopters around the world. When casualties find themselves inaccessible to land or air ambulances, SAR helicopter (SARH) crews are called upon to care for, extricate and rapidly transport patients to places of definitive care or safety (Howes et al, 2011). While the majority (around 80%) of their patients are victims of traumatic injury (Dykes et al, 2009; Sherren et al, 2013; Meadley et al, 2015), they are also called upon to assist those presenting with acute coronary syndromes. Despite the recent recognition of the search and rescue technical crewmember role by the College of Paramedics (2015: 36), the specifics of the profession remain unfamiliar to most.
Each SARH mission presents its own unique challenges due to numerous dynamic aviation, rescue and clinical considerations. The aim of this article is to provide an insight into the emerging role of the SARH paramedic by highlighting and critically analysing the considerations they are faced with when called to a cardiac patient on the mountainside. It will begin by revising the pathophysiology of acute myocardial infarctions and the importance of timely reperfusion. The article will then progress by highlighting and discussing the merits of, and the barriers to, the available cardiac care investigations and recommended treatment pathways in paramedic practice. The final section will explore an aspect previously considered outside the remit of the SARH paramedic: healthcare promotion and the rehabilitation process.
Background: the pathophysiology of myocardial infarctions
Cardiovascular disease (CVD) is a non-specific phrase used to describe diseases of the heart and circulation. The World Health Organization (WHO) estimates that CVD is the leading cause of death in the world, responsible for over 17.5 million deaths each year (WHO, 2015). According to the British Heart Foundation (BHF), around half of the deaths from CVD in the UK can be attributed to coronary heart disease (CHD) (BHF, 2015). Despite the number of deaths from CVD in the UK reducing by half between 1961 and 2009 (Scarborough et al, 2011), CHD remains the UKs single biggest killer (BHF, 2015).
The underlying disease process responsible for the majority of CVDs is atherosclerosis (WHO, 2011). Atherosclerosis is a generic term for the progressive and degenerative thickening of the arteries (see Figure 1). There are several risk-factors that promote atherosclerosis. Some of the significant contributors include smoking, an unhealthy diet and physical inactivity (BHF, 2015; WHO, 2015)— all of which appear to be behavioural choices.
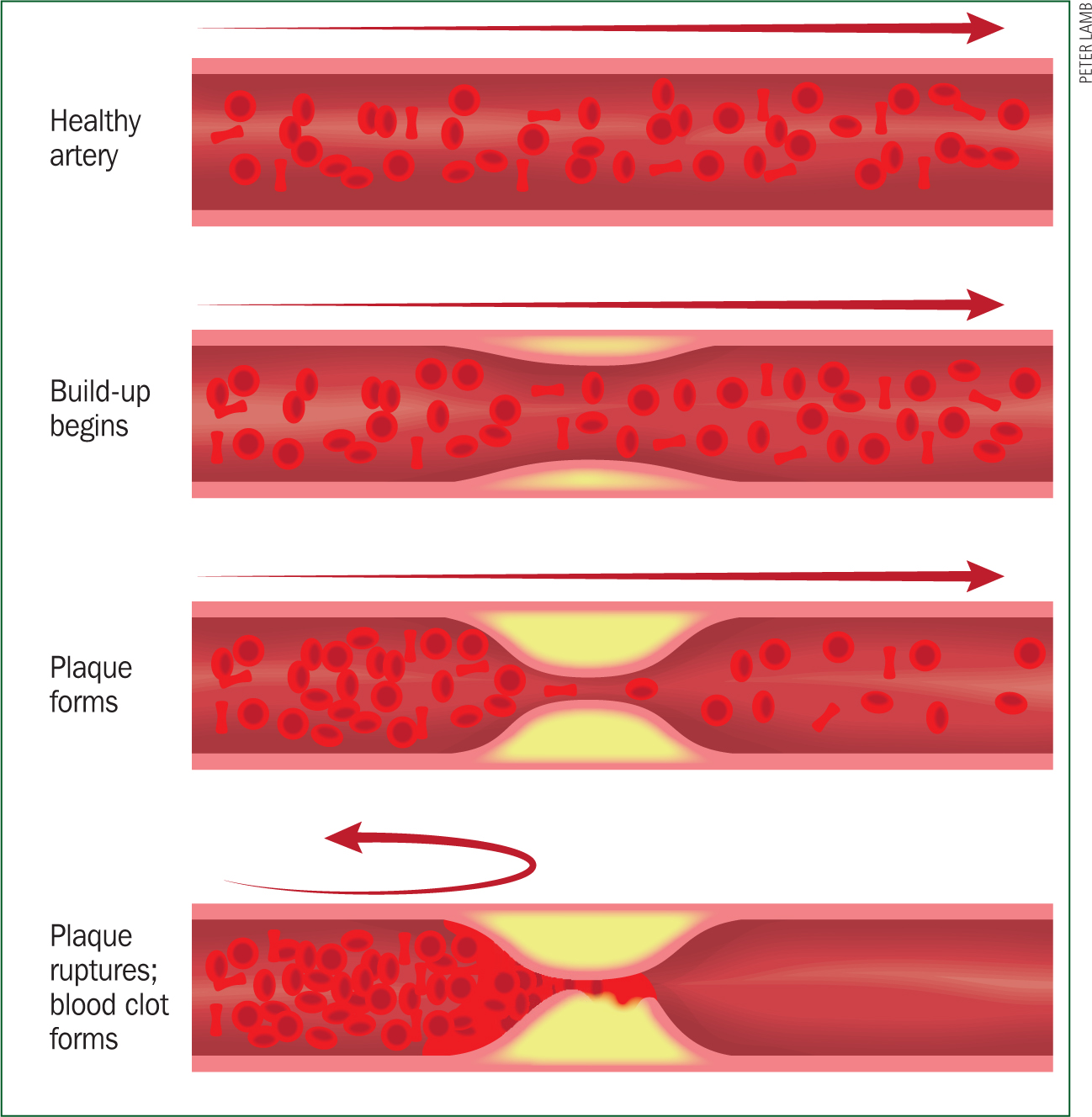
The National Institute for Health and Care Excellence (NICE) (2013) describes coronary atherosclerosis in more detail as the accumulation of protruding, elevated white lesions (plaques) within the relatively small bores of the coronary arteries. These plaques consist of a fibrous outer layer surrounding a lipid core. Blood flow over a plaque with a high lipid concentration and an unstable (thinner) cap can cause it to rupture. Platelets now accumulate around the newly exposed cholesterol core and a thrombus is formed. When a persistent and complete occlusion of a coronary artery by a thrombus occurs, blood flow and thus the delivery of oxygen to the myocardium distal to the blockage is impeded. Failure to resolve a blockage results in necrosis of the affected myocardium. This pathophysiology is referred to as a myocardial infarction (MI). Following complete occlusion of a coronary artery, an abnormality seen on the electrocardiogram (ECG) is elevation of the ST-segment. Hence, it is referred to as an ST-segment elevation myocardial infarction (STEMI).
The 12-lead ECG in SAR paramedic practice
Most deaths from CHD are caused by an acute MI (BHF, 2015). When one strikes, 50% of potentially salvageable myocardium is lost within 1 hour, two thirds is lost within 3 hours (NICE, 2013). ‘Time is muscle’ and muscle is life (NICE, 2013)—for both the SARH paramedic and their patient, the clock is ticking! Other than resuscitation from cardiac arrest, the most significant determinant in reducing mortality is the speed at which coronary blood flow can be re-established (Smith et al, 2010; NICE, 2013). Early reperfusion depends on a timely diagnosis, the cornerstone of which is the 12-lead ECG. The recent transition from a predominantly military SAR service to a civilian contracted one in the UK has brought with it the acquisition of a 12-lead ECG capability on SAR helicopters. The pre-hospital 12-lead ECGs role in the diagnosis of an acute STEMI is vital in enabling timely access to the preferred reperfusion treatments: percutaneous coronary intervention (PCI) and thrombolysis (TL) (NICE, 2013).
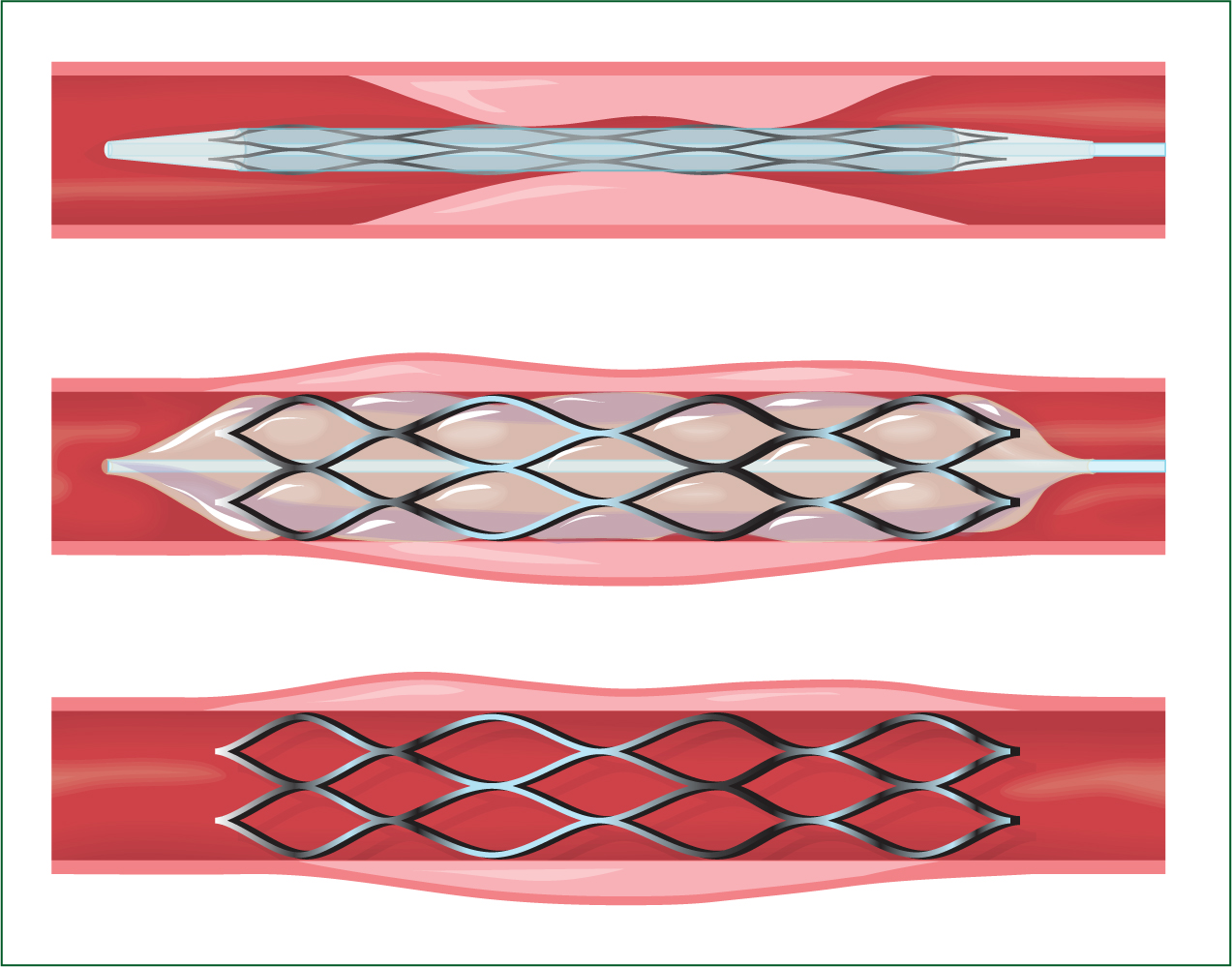
PCI is only available in specialist, tertiary centres and involves the introduction of a fine, guide-wire into an occluded coronary artery via the patients groin or wrist. A thrombectomy device is then advanced over the wire and the thrombus is mechanically aspirated. The device is removed and a balloon/stent is advanced and left in place to open up the artery (Figure 2). When this procedure is performed as the initial reperfusion treatment, it is referred to as a primary PCI (pPCI). Due to its high success rate and low risk rate in comparison to TL, pPCI is the treatment of choice for those diagnosed with a STEMI (NICE, 2013). The Association of Ambulance Chief Executives (AACE) (2013) have embraced the NICE (2013) guidelines and empowered paramedics to bypass local emergency departments (EDs) in favour of direct transportation to PCI centres. This enables timelier access to pPCI for those meeting a certain criteria. To facilitate this the pre-hospital 12-lead ECG is imperative.
If bypass to a PCI centre from scene is not possible, an alternative reperfusion method for the STEMI patient is TL. This involves the introduction of a thrombolytic agent to pharmacologically break down the offending thrombus. At the time of writing the SAR paramedics' formulary in the UK does not contain TL drugs. When bypass is not possible, SARH paramedics employ a ‘scoop and run’ strategy to rapidly transport their patients to the nearest ED for TL. In these circumstances the pre-hospital ECG could be misconceived as an unnecessary waste of time as it does not directly alter the SARH paramedic's immediate provision of care. But this is certainly not the case, the additional time spent on scene is justifiable. A pre-hospital STEMI diagnosis combined with a hospital pre-alert enables the ED staff to prepare for the arrival of the STEMI patient and administer timelier TL (Figgis et al, 2010). In comparison, the additional on-scene time is rendered insignificant as the overall onset-to-reperfusion time is still reduced (Figgis et al, 2010). Pre-hospital ECGs can also provide evidence of the evolutionary patterns indicative of MIs (College of Paramedics and American Academy of Orthopaedic Surgeons, 2014), they are also useful for pre- and post-reperfusion therapy analysis.
But, performing a 12-lead ECG in the SAR environment has its difficulties. SARH paramedic practice is unforgiving, conducted in a context fraught with chaos, danger and uncontrollable elements. During a SARH mission (by definition) injured or ill patients need treating and rescuing from austere, inaccessible locations. In extremis, taking time to perform a 12-lead ECG on scene may result in a missed opportunity for rescue due to aircraft, weather or fuel limitations. Ironically in these circumstances, focusing purely on clinical considerations may prove detrimental to casualty care. The urge to do so must be resisted, otherwise the patient may face a lengthy carry down the mountain by ground parties. If this occurs, by the time they reach a hospital, the window for timely reperfusion treatment may have passed and the SARH paramedic may themselves require assistance, calling on ground parties to escort them safely down the mountain. Overall mission success demands a holistic approach to the management of the clinical, aviation and rescue considerations.
The skill of performing and interpreting an ECG also presents significant challenges during rescue missions. Procedural guidelines suggest that the ECG is a simple investigation during which the patient should be relaxed and comfortable to reduce artefact (Gregory and Mursell, 2010). During a mountain rescue mission this is often challenging and not always possible. Casualties may be in precarious positions, wearing saturated clothing in gale force winds, shivering in temperatures below freezing. The prospect of being winched up around 300 ft to a hovering helicopter only exacerbates the situation for the already anxious, fearful patient. Sometimes just getting the ECG machine to the patient is challenging on the mountain. Winching down with a portable (yet still cumbersome) ECG machine can be impossible in hazardous conditions. Although in-flight ECGs are possible, a SAR helicopter is a turbulent, vibrating platform which is not conducive to obtaining an accurate ECG trace.
Patients not presenting with typical retrosternal chest pain make up around 30% of STEMI cases (Steg et al, 2012). These are typically older patients, women and diabetics (Steg et al, 2012; AACE, 2013). Thygesen et al (2007) describe common ECG pitfalls which mimic ischaemia or infarction, such as a left bundle branch block or pericarditis. These factors compound to further exacerbate difficulties in making a pre-hospital diagnosis of a STEMI. These difficulties can be overcome with training and regular exposure to ECG mimics (Huitema et al, 2014). But the predominantly trauma-orientated role of the SARH paramedic makes this challenging. Technological advances on modern helicopters offer an alternative solution. The advent of a data transmission capability via Bluetooth and a Wi-Fi ‘hotspot’ enables ECG telemetry from the aircraft. Already pioneered by their domestic paramedic colleagues, this provides the ability to collaborate with other healthcare professionals who posess a more advanced ECG diagnostic skillset.
Utilising this option not only promotes identification of those patients requiring reperfusion, but significantly in the case of the STEMI mimic, it reduces the number of false-positives (Davis et al, 2007; McLean et al, 2008). However, using this capability requires further consideration of the time constraints imposed by weather or fuel restrictions. Additionally, high cruising speeds of modern helicopters mean that the aircraft may be capable of reaching several appropriate hospitals (including pPCI centres) before the data can be transmitted, analysed and an answer communicated.
An investigation by Figgis et al (2010) concluded that only 20% of patients presenting to UK ambulance paramedics with chest pain had a pre-hospital 12-lead ECG recorded. Of the paramedics surveyed, 27.6% stated they had received insufficient training to perform and interpret a 12-lead ECG; 64% cited the same reason for their inability to interpret ECG abnormalities. This study had a small sample size taken from one region rendering its external validity compromised. It is not necessarily a true reflection of UK paramedic practice as a whole, but it does reemphasise the training implications already highlighted. Beygui et al (2015) recommend that specific training in ECG interpretation should be mandatory for those involved in the care of STEMI patients. Whitbread et al (2002) concluded that with sufficient training, UK paramedics are comparable to emergency department doctors in diagnosing STEMIs from a 12-lead ECG. They are able to diagnose with a sensitivity of 97% and a specificity of 91% (Whitbread et al, 2002). Provided they are adequately trained, SARH paramedics, like their domestic counterparts, can act as a vital timely filter for the activation of reperfusion pathways.


Thrombolysis in local EDs versus bypass to a PCI centre
Ultimately, the reperfusion strategies available to the STEMI patient on the mountain are determined by the SAR paramedic's choice of destination hospital. The complexities and dynamics of a SAR mission often hinder strict adherence to clinical guidelines. But this does not excuse guideline non-adherence as the default option, the decision not to bypass to a PCI centre must be justifiable and on a case-by-case basis.
Once a STEMI diagnosis has been obtained, the greatest barriers to the SARH paramedic adhering to the AACE (2013) PCI centre bypass guidelines are the aviation and strategic considerations. The primary role of a SAR helicopter is to rescue those in urgent need that other agencies cannot reach within the required timescale; clinical care can often be relegated to an ancillary consideration. Bypass to a PCI centre may result in a significant, additional delay (over an hour) in the asset being available for re-tasking. Unlike the ambulance service, the nearest comparable, covering asset is often the neighbouring SAR base over 100 miles away. For some casualties (such as those drowning), timely rescue by a SARH makes the difference between life and death. SARH paramedics may be asked to conduct rapid, in-flight triage when information about other, life-saving tasking is received. They must weigh up the benefits gained through facilitating pPCI in preference to TL for one patient, against the odds of other persons requiring timely rescue by a SARH.
While weather and fuel restrictions also hamper the ability to bypass, infrastructure can also be limiting. Many PCI centres do not have a dedicated helicopter landing site (HLS) suitable for a SAR aircraft on-site. A recent review estimated that 60% of hospitals in the UK have inadequate helicopter landing facilities (Association of Air Ambulances, 2014). The subsequent secondary ambulance transfer from a nearby ‘field’ HLS can incur significant delays. Although pPCI is the preferred reperfusion method, TL at local EDs can offer a more favourable alternative from purely an aviation perspective.
To produce their STEMI guideline, the NICE (2013) conducted a clinical review comparing the incremental benefits of pPCI over TL. They concluded that, despite pPCI related time delays, it is both cost effective and feasible; it is the preferred treatment for those meeting its criteria and should be administered in a timely manner (NICE, 2013). But the evidence is not unanimous for this ‘one-size-fits-all’ guideline; a detailed review suggests no single pathway is optimal for all patients, in all situations.
Defining the equipoise for pPCI and TL is complex. One determinant appears to be patient age and profile risk (Pinto et al, 2006; Tarantini et al, 2009). A review of the evidence conducted by Widimsky (2009) suggests that patients older than 65 years of age, or with a higher Killip class (higher mortality risk), should be treated with pPCI. But those younger than 65 years, with a low Killip class, only appear to gain significant benefits from pPCI if the related time delay is less than 35 minutes (Widimsky, 2009). For this subgroup presenting on the mountain, where pPCI related time delays may be significant, TL appears a suitable alterative. However, Widimsky (2009) admits the small numbers in this subgroup cast doubts on his conclusions. The NICE (2013) acknowledge this and recommend further investigation through a randomised controlled trial to compare the outcomes between TL and pPCI for those presenting within 1 hour of symptoms.
Although TL at the nearest ED is favourable from purely an aviation perspective, when compared to pPCI, it is blighted by clinical contraindications and complications. While TL usually dissolves the thrombus, the underlying atherosclerotic plaque often remains and reocclusion is common (Schofield, 2011). In around 5% of cases this leads to reinfarction and a poor associated outcome (Gibson et al, 2003). It is also less successful in sufficiently opening the effected artery (Schofield, 2011). Widimsky et al (2009) state that mechanical (pPCI) reperfusion rates are circa 90% in comparison to a pharmacological (TL) reperfusion rate of circa 50%. The AACE (2013) re-iterates this difference in success rates in its TL guideline. It states that TL in the field should not be considered the end of emergency care, as these patients still require rapid transfer to an appropriate hospital to prevent re-infarction and assess the need for rescue PCI.
As a non-specific treatment, TL also predisposes patients to a higher risk of haemorrhagic stroke and bleeding (Schofield, 2011; Beygui et al, 2015). Some patients are exposed to an increased risk of intracranial haemorrhage (0.2–1%) (Califf et al, 1992) without gaining significant benefit. When this risk overbalances the expected benefit, TL is contraindicated (Beygui et al, 2015). For these patients, any apparent initial benefit gained from rapid transportation from mountainside to a local ED is no longer applicable. These patients attract a high mortality rate; the AACE (2013) specifically emphasises the need for direct transportation to a pPCI centre for this subgroup, whenever possible. From a purely clinical perspective, timely pPCI is the treatment of choice.
Rehabilitation
Regardless of reperfusion therapy, cardiac rehabilitation (CR) is crucial to restoring cardiac patients to optimal health and psychosocial function; it begins from the point of first medical contact and can continue for the rest of the person's life (Grove, 2011).
Life-threatening cardiac events induce feelings of fear, hopelessness, anxiety and ultimately depression. Approximately 39% of cardiac patients cite ‘a lack of interest’ or ‘refusal’ as their main reason for not participating in CR programmes (Doherty et al, 2014). The National Service Framework for Coronary Heart Disease recommends that a patient's psychological needs are assessed and addressed throughout the four stages of CR (Department of Health, 2000). The ability of patients to manage these psychological difficulties induced by life-threatening cardiac events remains vital to the success of CR (Doherty et al, 2014). This is a multidisciplinary responsibility and should begin early for all patient groups (Doherty et al, 2014).
The evolving role of the paramedic now extends beyond that of a purely reactive profession that provides care and transportation. The paramedics' registering body, the Health and Care Professions Council (HCPC), now embraces the concept of healthcare promotion for paramedics (HCPC, 2014). While the back of a SARH is not traditionally regarded as a suitable venue for the promotion of health care and the rehabilitations process, meeting the psychological needs of the patient in the pre-hospital setting might be crucial to their subsequent perception of the emergency. The rehabilitation process can begin on the way to hospital by reassuring the casualty that although the situation is serious, it is not hopeless and that with optimism, determination and adherence to the CR programme there is no reason they will not make a full recovery. Assessing and addressing a patient's psychological needs immediately may be relevant to the likelihood of the patient attending rehabilitation.
Conclusions
CHD is the UKs single biggest killer. When a person falls victim of a STEMI on the mountainside, timely reperfusion is imperative. But for the SARH paramedic, the patients' immediate clinical requirements are not the only consideration. One of the most highly prized attributes of the SARH paramedic is not their abilities as a clinician, but their ability to manage the competing, cumulative considerations during a SARH mission. It is often challenging, sometimes impossible, to comply with the recommended clinical guidelines.
Cardiac care on the mountainside demands that practitioners are neither uncompromising slaves to clinical protocol, nor do they ignore guidelines without justification. SAR clinicians must evaluate the evidence behind clinical guidelines for validity, applicability and usability, while concurrently considering the aviation and rescue implications of each SARH mission on a case-by-case basis. Only after considering these elements can they make informed decisions on ‘what, when and where’ with regards to investigations, treatments and destination hospitals for the cardiac patient. Although healthcare promotion and CR has not traditionally been within the SAR paramedics remit, addressing a patient's psychological needs early, increases their likelihood of participating in rehabilitation programmes.
Key Points
Conflict of interest: none declared