The National Health Services (NHS) accounts for 5 % of all road traffic in England, with staff, patients and visitors travelling over 20 billion kilometres annually by car (GrEAN, 2011). Changes in UK Governmental policy are encouraging a shift away from emergency care and towards urgent (pre-hospital) care by providing assessment, diagnosis and treatment for patients in their own homes. These changes are increasing the number of solo responders with enhanced clinical skills (Department of Health, 2006).
Under the Climate Change Act (2008) the UK Government has implemented legislation to regulate and reduce carbon emissions. In order for these initiatives to be successful, low carbon transport must become a genuine, viable and attractive option for services and businesses as well as ordinary citizens. The Green Environment Ambulance Network (GrEAN) is a network of UK ambulance services working to reduce the collective carbon footprint of the ambulance Trusts. They have been investigating alternative fuels for future ambulance fleets including electric vehicle technology. Ambulance fleets have considered the aerodynamics, weight and fuel efficiency of the NHS vehicles with an ‘Eco Driving’ initiative finding that Trusts could save up to £1.5 million per annum by managing driving behaviour leading to reduced fuel use, fewer accidents and lower maintenance costs, without sacrificing the standard of care (GrEAN, 2011).
FEVA is a proof of concept study to explore the introduction of low carbon electric solo responder vehicles as part of the ambulance fleet. The study aimed to continue research conducted in previous projects investigating emergency ambulance design (Hignett et al. 2009), pre-hospital care (Hignett et al. 2010; 2011), portable clinical equipment (CURE; Hignett et al, 2012) and the design of compact lightweight vehicles (Disruptive Technologies in Low Carbon Vehicles (Smith et al, 2011).
The objectives were to:
Method
Mock up
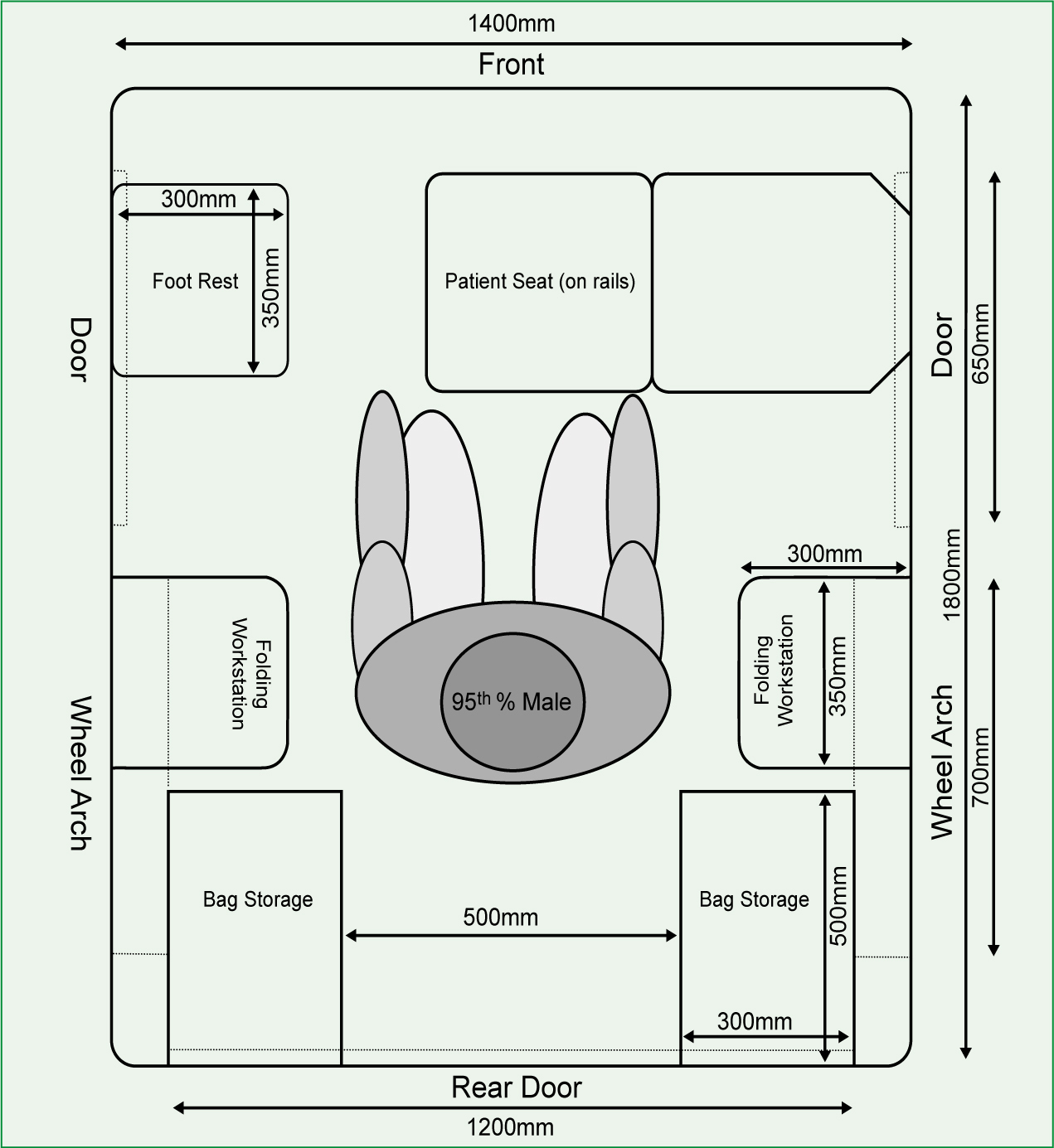
The FEVA interior (Figure 1) was designed to provide a treatment area for solo response vehicles with storage units for equipment bags, patient and clinician seats as well as lay down space as work stations based on previous research (Hignett et al, 2012) and UK population anthropometric data (Pheasant and Haslegrave, 2006). The mock-up was designed to a minimum specification to allow for regional variations.
Participants
The FEVA mobile mock-up was taken to five ambulance Trusts across England: South West, East of England, East Midlands, South Central and Yorkshire. Participants included solo responders (emergency care practitioners and paramedics), fleet and operational managers and members of the GrEAN committee.
Data collection
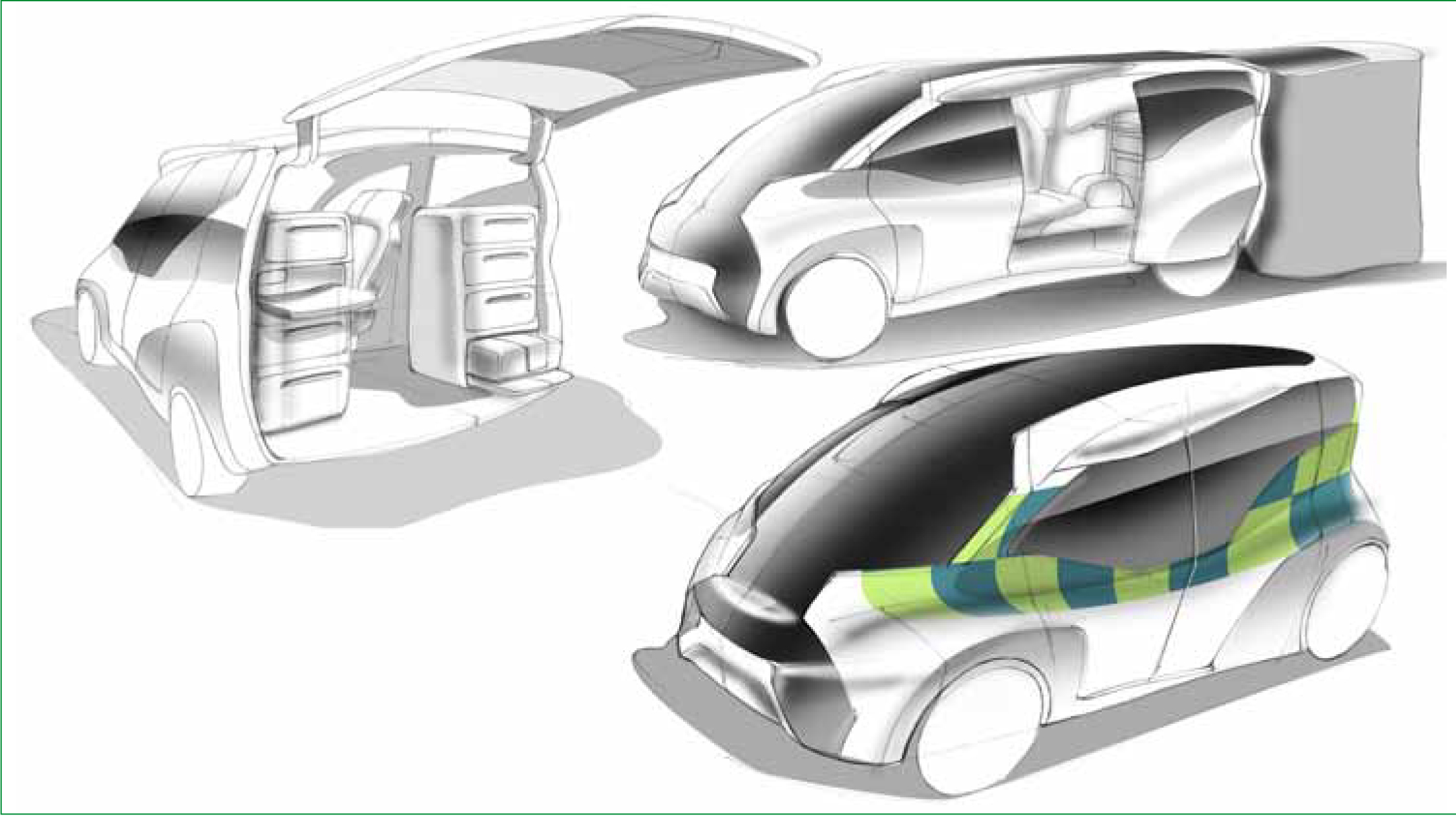
A two stage approach was used to firstly discuss the overall electric vehicle concept (requirements and expectations) and secondly evaluate the proposed interior design/layout (treatment area). Data were collected in the first stage using a word mapping approach (Wilson et al. 2005) in group discussions with visualisation sketches to give an impression of the appearance of the vehicle (Figure 2). The participants were asked to consider patient and clinician perspectives by exploring the interior of the vehicle and using the patient and clinician seats (treatment area evaluation).
The second stage used individual interviews to explore specific issues from stage 1 in more detail (Table 1).
Results
The data from the word map (Figure 3) were grouped to develop the interview proforma (Table 1) for the second stage of data collection. The interview data were analysed to identify common themes for the overall concept and treatment area evaluation (Table 2).
Discussion
The first aim of this study was to understand the expectations for low carbon electric vehicles in the emergency services. Generally, the concept was positively received with recognition of the need for low carbon transportation with some specific concerns about the adoption of electric vehicles.
The issues focused on the range (the distance that could be travelled on a single charge) and the time taken to re-charge the vehicle between dispatches. With current technology it was suggested that electric vehicles could be introduced with a limited scope of use, for example in urban city centres, for on-site treatment vehicles (including events) and within small communities with shorter daily distances to reduce the distances travelled and provide overnight chargi ng capabilities.
The Nissan Leaf (comparable to the NV200 van for performance) has a single-charge range of 70–130 miles depending on driving patterns and environmental conditions, with a top speed of 90 mph (Nissan, 2012). Future technology trends indicate lithium-ion battery improvements over the next decade will extend the range to over 300 miles (Biello, 2012) making the vehicles’ range comparable to internal combustion engine models and that new lithium-air batteries will enable electric vehicles to be suitable for almost all driving scenarios (Birke et al. 2010). It was felt that when these operational targets are achieved, electric vehicles could be used as solo response vehicles.
‘…once the range of electric vehicles reaches 300 miles for a single charge, this [FEVA] could become a very real possibility’.
Even with technology advances, additional infrastructure will be needed for electric vehicles to operate in the emergency services, for example charging facilities at ambulance stations, hospitals and standby locations to maximise the possibilities of quick charge times of 10–30 mins (Humphries, 2011). Further advances being considered include ‘wireless charging’ with the vehicle parked over an induction floor-mounted plate which could be used at ambulance standby locations to keep vehicles topped up (Moskvitch, 2012).
‘…one of the themes related to acceptance by paramedics due to limited knowledge about the capabilities of current and future electric vehicles.’
The cost of purchasing electric vehicles was identified as a theme (business case). There are government carbon benefit allowances that can reduce the initial cost of purchasing an electric vehicle. Although long-term benefits were noted by many of the participants (efficiency of running an electric vehicle and lower maintenance costs), until range is increased and charging time decreased it will be difficult to make a business case for electric vehicles:
‘…at the moment the technology seems to be in a ‘Macintosh’ era, whereas we need to be in the ‘iPad’ stage before the full benefits of electric vehicles can be realised’. At present it was felt that electric vehicles would be too expensive, even with lower operational and maintenance costs, ‘need to consider the full carbon life cycle and the associated costs of recycling batteries’.
When considering implementation, one of the themes related to acceptance by paramedics due to limited knowledge about the capabilities of current and future electric vehicles. This included the lack of engine noise; this has been discussed extensively and is likely to increase in the future in response to lobbying from the visually impaired community (Green Car Reports, 2012). There was also a perception that:
‘…electric vehicles were weaker than normal cars’
so demonstrations and trials would be needed to improve the perception of electric vehicle performance. It was suggested that the FEVA vehicle could be introduced into the ambulance service as a flexible vehicle for solo response possibly as a specialist community daytime service (blood donations or vaccination) for a trial. It was felt that there were benefits to standardising the interior to help manage equipment and consumable logistics:
‘crews tend to stock the vehicles with extra equipment based on personal preference—if there is space it will be filled’
It was felt that the current standards for staffing and equipment in solo response vehicles would be appropriate with local variations for geographical differences, for example, rural rather than urban environments.
The second aim was achieved by designing, building and evaluating a mock-up of the FEVA interior as a solo responder vehicle. It was generally felt that a mobile treatment area would improve the patient experience and provide greater privacy and dignity for the patient:
‘this has the potential to be great by providing improved treatment to the patient close to their homes without the needs for onward care’
For the clinician, the treatment area would provide a more functional working environment in which more clinical tasks could be conducted (for example, suturing). Standardisation and modularisation were key design requirements for equipment and consumables based on previous research (Hignett et al, 2007). The rear storage shelving (Figure 1) with the clearly labelled CURE bags was very positively received and provided access to equipment and consumables from within and outside the vehicle. Each shelving unit was designed to accommodate a CURE response bag (standardised size and footprint) with an additional storage for extra equipment. It was recommended that there should be a separate response/grab (emergency) bag for use when responding to a patient away from the vehicle. When treating a patient in the vehicle, the equipment and consumables from the CURE bags and shelving units were felt to be well organised and accessible for the clinician; additional work stations (lay down space) were recommended for smaller items. The movable seat enabled the clinician to be seated in a suitable position to both reach equipment/consumables and attend the patient. To access both sides of the patient it was suggested that the patient seat would need to swivel through 180°.
To improve patient dignity, a bulkhead between the treatment area and the front seats or a curtain would be needed to prevent observation through the windscreen.
The treatment area was designed to have two points of exit (rear door and side door) to ensure the safety of the patient and clinician and allow for rapid egress. It was noted that elderly patients might have difficulty accessing the vehicle even with steps due to the low ceiling height. This could also affect performance within the treatment area especially if the paramedic needed access to the patient's head for examination or treatment. Possible solutions could include a roof-extension (similar to a caravan) or to expand the design of the FEVA concept into a vehicle platform with a larger rear section (for example, Mercedes Vito or VW Shuttle/Transporter).
Clinical activities with fine detailed work would also benefit from a moveable light and spot lights on the ceiling.
Irrespective of the powertrain, if vehicles with the improved treatment area were introduced then fewer patients would require transport to hospital. While this may have clinical benefits by reducing waiting times, it would also have direct benefits in terms of carbon emissions by reducing the distances driven. Should this be coupled with an electric powertrain, as the scenario in this study, the range requirements would be reduced, increasing viability of an electrically powered vehicle.
Conclusions
Ambulance trusts have acknowledged the need to lower carbon emissions within the vehicle fleets but there is some hesitation in using low carbon electric vehicles due to the cost of purchasing vehicles and ancillary equipment. Despite acknowledging the long term benefits that electric vehicles offer with lower operating and maintenance costs, the current status of battery technology is seen to be a barrier for fleet services.
‘At the moment the technology seems to be in a ‘Macintosh’ era whereas we need to be in the ‘iPad’ stage before the full benefits of electric vehicles can be realised’.
When the performance of electric vehicles becomes more comparable with internal combustion engine vehicles, there is likely to be greater support for low carbon electric ambulance vehicles. The research on standardisation and modularisation has made a significant impact on future ambulance design to improve both clinical efficiency and patient experience. This now needs to be transferred to solo response vehicles to optimise vehicle performance, clinical service provision and patient satisfaction.