Emergency services in England ranging from pre-hospital care all the way to intensive care capacity are always busy. Patient care requires an efficient and seamless service where demands can be met. Individual trauma events are unforeseeable events and, as such, predictions as to the volume of admissions over a particular calendar period are often difficult, making service planning and provision challenging and sometimes inefficient.
Healthcare professionals involved with trauma admissions (paramedics, emergency departments, trauma and orthopaedic services) have long been been aware of a repetitive annual pattern for trauma. There has been an admission influx during the summer months, when the weather is better and the sun shines for longer, and this is especially true for paediatric admissions. Hazardous weather conditions have also been linked to increased road traffic collisions and hence trauma. Furthermore, cold icy conditions make people more prone to accidents, both from road traffic collisions and from falls, especially in the elderly population. One can therefore hypothesise that weather and weather changes can be responsible for variations in trauma admissions. But the question remains as to whether evidence exists to support this?
At our department the effect of seasonal variation on major trauma influx has been the focus of clinical research. We have studied the data from a cross sectional study of patients arriving at 21 selected ED located across England between 1 January 1996 and 31 December 2006. This included 59 617 patients, making the study by far the most comprehensive and most conclusive the field (Parsons et al. 2010). Our study, along with others, have shown the significance of weather variation on trauma admissions, however, these results can differ.
When referring to trauma admissions the population should be divided into paediatric and adult trauma, as there seems to be a marked variation in effect on these patient groups.
Methods
A systematic search for relevant studies was undertaken using Medline, EMBASE and Cochrane databases. Studies from 1990 to 2011 were included. The MESH terms used for the search included: trauma admissions, seasonal variations, paediatric trauma admissions, weather forecast, road traffic collisions. The searches returned 25 results. Most of these are retrospective data collections from specific trauma centres/areas admissions, which are subsequently correlated to the specific weather characteristics of that day. A trend was identified and presented. There was one cross sectional study involving 21 ED running over 11 years.
A trend was identified and presented. When referring to trauma, admissions the population was divided into paediatric and adult trauma, as there seems to be a marked variation in effect on these patient groups.
‘With regards to paediatric admissions, the most common injury is distal radial fractures (48 %), followed by supracondylar fractures of the humerus (9 %) and humeral fractures (8 %)…’
Paediatric trauma
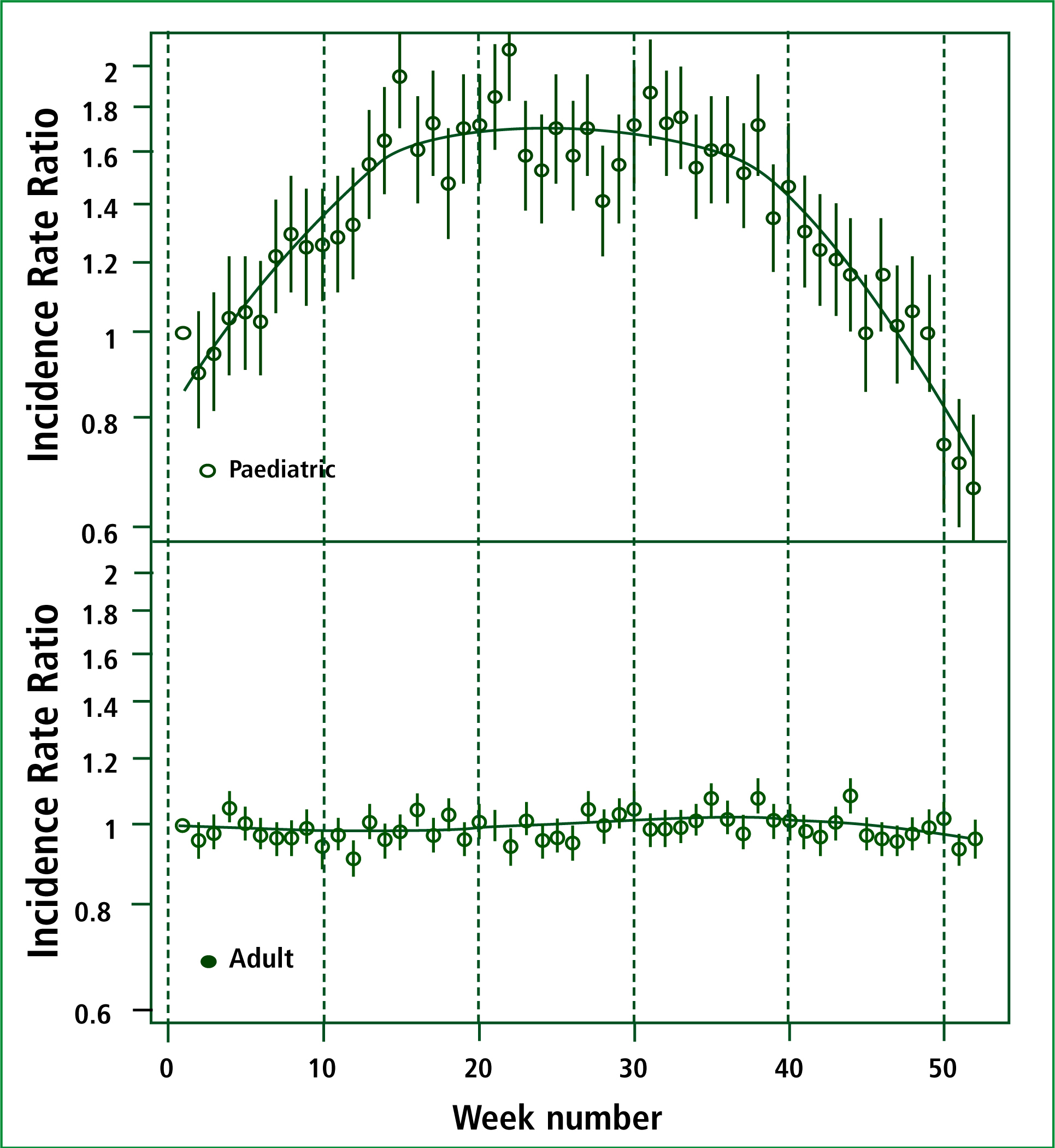
With regards to paediatric admissions, the commonest injury is distal radial fractures (48 %), followed by supracondylar fractures of the humerus (9 %) and humeral fractures (8 %). The ratio of boys to girls is 1.6:1 with boys being more likely to sustain an injury. The mean injury age for boys appears to be higher than girls (8.2 vs 7.6) (Masterson et al. 1993). The literature shows evidence suggesting that more daylight and higher temperatures result in more trauma admissions in this group. During the summer weeks paediatric trauma admissions are increased by up to 60 % (IRR 1.6) (Masterson et al. 1993; Abe et al, 2008; Parsons et al. 2010). Atherton et al (2005) have shown that an increase of 5 º C in daily temperature results in a rise of paediatric admissions by 11 %. Furthermore they demonstrate that every additional hour of sunshine results to an additional rate of 4 % (Macgregor et al, 2003) however, argue that higher temperature alone is not responsible for a surge in paediatric trauma admissions, and the only correlation his group could find is increased sunshine (Macgregor et al, 2003).
Parsons et al (2010) supported this and identified the effect of school holidays and weekly variation. The authors demonstrate a consistent pattern showing increased admissions during school holidays by an estimated 6 %. Furthermore they identified a weekly pattern where admissions are the lowest on Tuesday (16 % lower) followed by gradual increase until the weekend.
The correlation of mean monthly rainfall and children's injuries was found to be very weakly negative (Rotstein et al. 1997).
Adult trauma
Clear association between seasonal hazardous conditions and road traffic collisions have been demonstrated, and is supported by police data (Edwards, 1999; Abe et al, 2008). The authors conducted their study in Tokyo, reviewing all the ambulance transport records from January to December 2005. This was correlated with hourly meteorological data during the same period. Their cohort included 226 339 patients. They identified a strong association in trauma admissions and increased rainfall (P < 0.01). They also linked increase in trauma with high temperature (P < 0.05) and holidays (P < 0.01).
Rising et al (2006) looked into the admissions of Louisville's Trauma Institute Registry data from July 1996 to January 2002. This included 8 269 patients, and they correlated this with the local forecast database. The authors concluded that maximum temperature over the preceding 24 hours and precipitation were significant in predicting adult trauma (P < 0.001). They have concluded a 5.25 % increase for a 10-degree difference in temperature. They also found a 60–78 % increase in the incidence for every inch of precipitation in the past three hours.
Atherton (2005), looked into the admissions to Leicester Royal Infirmary for 1996. Their conclusions are in line with the above. They have, however, made an important exception; as a subgroup of patients, presenting with low energy proximal femoral fractures appeared to exhibit no variation in incidence with weather variations. This is contradicted by (Crawford et al. 2003) who identified a statistically significant seasonal variation with hip fractures. He identified that more hip fractures (P=0.002) occur during the winter. Furthermore the authors claim an increase in extra-capsular fractures (P=0.006) and tendency to higher mortality (Crawford and Parker, 2003)
Parsons et al (2010) conducted a cross sectional study of patients arriving at 21 selected ED located across England between 1 January 1996 and 31 December 2006. This included 59 617 patients and the data was correlated with with meteorological data. The authors found with the seasonal variation as discussed above, including the effect of rainfall on admissions. In addition, the correlation of snow and sleet was highlighted (7.9 % increase in admissions).
The presence of night frost seems to be important as well, as the authors noticed a consistently increased rate in admissions by 2.2 %. The authors have not however identified a statistically significant variation in admissions during the summer months as seen for the paediatric group. The authors support that, similar to paediatric admissions, adult trauma shows a consistent variation during the week showing a trough in admissions on Tuesdays (16 %) compared to a peak on Saturdays. A significant surge of admissions appears on Saturdays compared to Fridays (11 %).
Discussion
We have presented a collection of studies, which recorded data on trauma admissions and their correlation with weather variation. Based on the evidence available, it is clear that weather affects the rate of trauma admissions. All the studies reviewed agree on that fact. Therefore the long held suspicions of healthcare providers are now clearly backed up by evidence. Beyond the moral reward of being proven right, does this lead us to any useful conclusions?
To do that one has to extrapolate the results. The fact that seasonal variations affect trauma influx on its own is not particularly useful. It should be analysed and the new knowledge gained should be directed appropriately towards improved patient care, efficiency and staff training.
Are we therefore clear of what we know? The strong correlation of paediatric admissions with summer conditions is clearly evident. Higher temperatures, more daylight and school holidays gives children more time to play outdoors and do those things that make them vulnerable to trauma. Maximum daily temperature and sunshine in adults has a less pronounced effect, which nevertheless is detectable, this again is probably secondary to increases in outdoor sporting activities, travel etc. In this group, adverse, hazardous weather conditions such as heavy rainfall and icy roads comprise another reason for an increase in major trauma. This can explain the increased risk for road traffic collisions.
A subgroup in the adult population should be mentioned here and this is the elderly group being admitted with falls and neck of femur fractures. Although there was a small variation in data, the general consensus is that there is an increase in number of admissions during the icy periods.
Weather forecasting has historically been inconsistent and unreliable, however the accuracy of both short and medium term forecasting continues to improve. It is reasonable to assume, therefore, that accurate weather forecasting can help in the correct allocation of healthcare resources. A project funded by the Department of Health was initiated between October 2000 and March 2001. This included monitoring real time activity in specified geographic areas, in conjunction with weather forecasts and twice weekly workload predictions. This resulted in an accuracy of 50 %, which could improve to 80 %. This translated saving £ 400 000 pounds for a single month at a single site (White, 2001).
An increase in forecasting accuracy will allow better resource planning for trauma care providers. However, the variation in trauma volume on different days of the week is already easily predictable and consistent. Care providers should incorporate in their staffing plans the weekly variation discussed above. This event in itself can make the system more efficient making sure that staff is used efficiently and when needed. This can further be reinforced by continuously using weather forecasting into the weakly and seasonal planning for the allocation of resources. This necessitates flexibility efficiency and teamwork.
‘Maximum daily temperature and sunshine in adults has a less pronounced effect, which nevertheless is detectable, this again is probably secondary to increases in outdoor sporting activities, travel…’
Workforce allocation is not the only field where predicting surges of trauma, and perhaps its nature can help. Education, teaching and training can also be directed and targeted. For example during the summer months training can be more focused around paediatric injuries. Refresher courses can run at the beginning of summer. Training rotations can be setup likewise and perhaps adjusted according to the specific needs of that particular period.
Conclusions
With the data analysed, it is clear therefore that trauma influx has strong association with weather variations as well as consistent weekly variations. It is easier to use the weekly variation patterns towards allocating services, as this is more consistent.
Weather and trauma are related and some of the associations are strong. The challenge is to respond to both short and medium term changes in weather so that, through planning, training and resource allocation, the best care can be delivered to our patients.
The NHS has been traditionally known for its rigidity and inability to adjust to change and the challenge is to be able to provide flexibility, this data provides a framework of how this can be achieved.