
Serious pelvic injuries are associated with a high mortality rate (Papakostidis and Giannoudis, 2009; Chesser et al, 2012), which has remained persistently high even with advances in hospital care. Hypovolaemia is often a significant contributing factor to these deaths (Lee and Porter, 2007; Papakostidis and Giannoudis, 2009). If haemorrhage from pelvic injuries could be controlled or reduced in the pre-hospital environment, then survival rates might increase.
Improved mortality has been seen with catastrophic haemorrhage from limb injuries after the introduction of the battlefield tourniquet and topical haemostatic dressings (D'Alleyrand et al, 2010). However, compared with bleeding from pelvic injuries, external haemorrhage is simple to recognise and the success of intervention easier to observe.
Pelvic binding devices provide a simple alternative to surgical fixators. These devices can be applied in the pre-hospital environment, potentially allowing control of unseen major haemorrhage (Chesser et al, 2012). This article reports the finding of a consensus meeting on the pre-hospital management of pelvic injuries held in March 2012 and examines the evidence associated with pelvic binding devices and their application.
Method of literature search
A review of the literature was undertaken prior to the consensus meeting. The Medline Database was searched using PubMed and Google Scholar was also used. The search terms were Pre-hospital management of pelvic injuries, Pelvic circumferential compression devices, pelvic binders, SAM pelvic sling, T-POD, PelvicBinder, Geneva belt and London pelvic sling. Further articles were identified from the references of retrieved articles. Manufacturers' websites were reviewed for further information regarding specific products.
Consensus outcomes
1. A pelvic binder is a treatment intervention rather than a packaging intervention and should be applied early
The initial management of any patient with a suspected pelvic injury must include the usual safety precautions. During scene assessment, visual clues to the mechanism of injury will help determine the likelihood of a pelvic injury.
The primary survey should deal with external catastrophic haemorrhage then any significant airway and/or breathing issues prior to circulatory assessment. If the patient is haemodynamically compromised with a significant mechanism suggestive of a pelvic injury, a pelvic binder should be applied.
Applying a pelvic binder early provides stability and allows clot formation. This may prevent ongoing haemorrhage and the often-lethal trauma-induced coagulopathy.
The consensus group emphasised that the pelvic binder is a treatment intervention rather than a packaging device and if the device is thought of as a haemorrhage control device this should promote early application.
2. A select group of patients may not need a binder applied
Pre-hospital diagnosis of a pelvic fracture can be extremely difficult (Lee and Porter, 2007). There is no obvious external bleeding and deformities can be difficult to detect. Grant 1990 found that ‘springing the pelvis’ had a poor sensitivity (59%) and specificity (71%).5 There is also concern that compressing the pelvis can cause further haemorrhage and as a result this technique is no longer recommended (Grant, 1990; Lee and Porter, 2007).
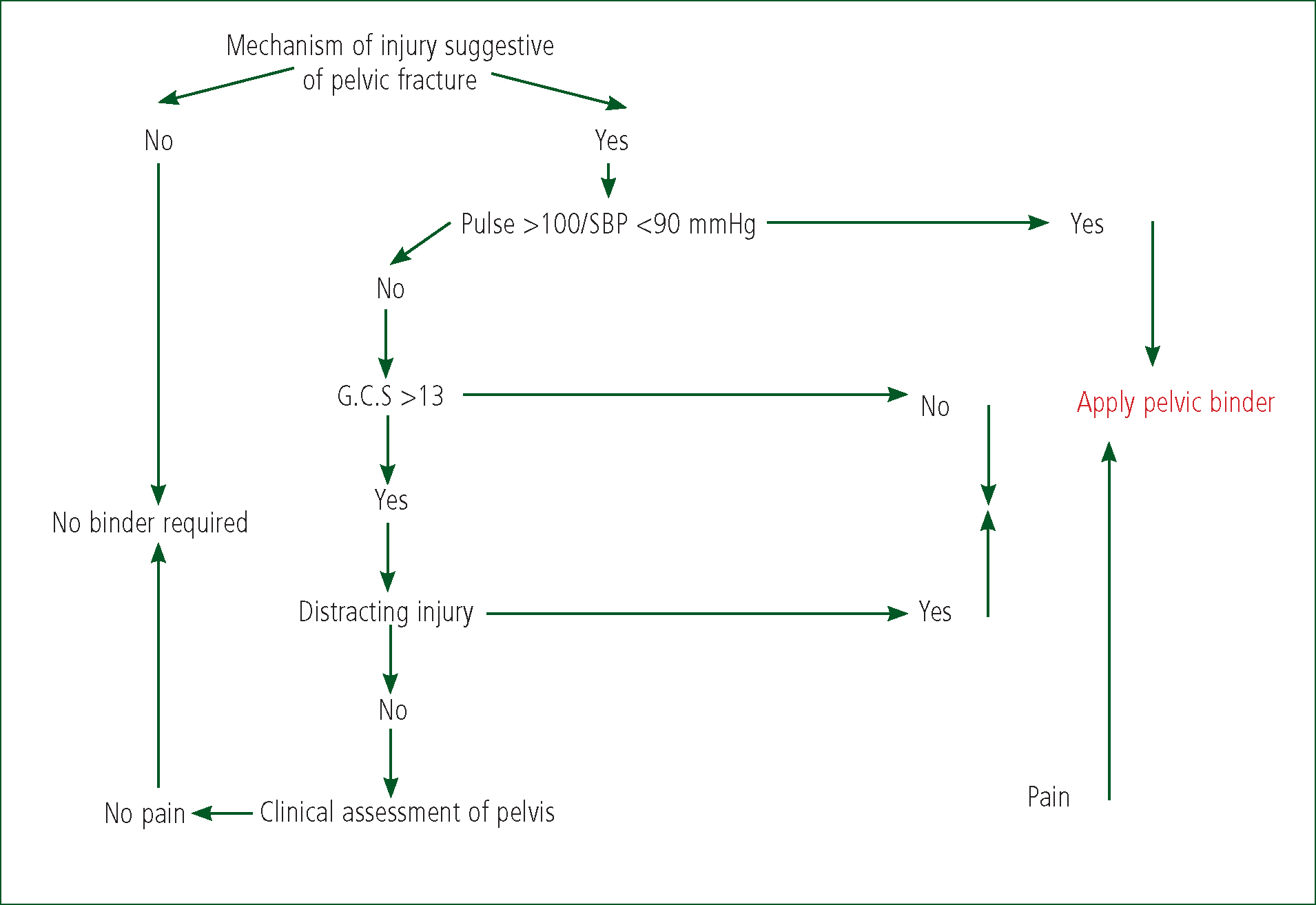
Significant pelvic trauma can be excluded from a small group of patients preventing the unnecessary use of pelvic binders.
These patients must be haemodynamically stable with a normal Glasgow Coma Scale (Sauerland et al, 2004; den Boer et al, 2011). The following flow diagram is an illustration of how patients can be stratified according to the risk of pelvic injury (Figure 1).
3. No one pelvic binder device can currently be recommended over another
The ideal pelvic binder should stabilise the pelvis in order to reduce haemorrhage and pain. It should be easy to apply, not cause further harm and allow radiological and surgical intervention without need for removal. In addition, it should not be too expensive to purchase or maintain.
A number of pelvic binding devices currently exist. There is limited evidence regarding their use in the pre-hospital environment. Cadaver and some clinical evidence suggest that pelvic stabilisation can be achieved with these devices (Bottlang et al, 2002a; 2002b; Bonner et al, 2011). A number of case series and reports suggest an improvement in haemodynamic stability and a reduction in blood transfusions after a pelvic binder has been applied (Simpson et al, 2002; Warme and Todd, 2002; Tan et al, 2010).
Currently, there is insufficient evidence to support one device over another. The two devices with the strongest evidence base are the SAM pelvic sling and T-POD devices.
Manufacturers of new devices should provide evidence that their device provides a similar level of stabilisation to these in cadaver models at least prior to them being made available for clinical use.
4. Adequate training must be provided to avoid misplacement of devices
There is evidence that misplacement of pelvic binders can reduce the degree of fracture reduction Bonner et al, 2010). It is important that pre-hospital providers are trained appropriately to optimise correct placement (Bonner et al, 2010.
While there is evidence that these devices are often incorrectly placed, this was felt to be a training issue rather than an inherent design fault. Pre-hospital providers must ensure that their members/employees are appropriately trained with clinical governance structures in place to provide constructive feedback.
5. Associated femoral fractures should also be reduced
Significant pelvic fractures require large energy transfers and are often associated with other lower limb bony injuries. There is no evidence that pelvic binders are harmful when applied to patients with proximal femur or acetabular fracture Chesser et al, 2012).
Patients who also have suspected or obvious femoral fractures should have these stabilised, ideally using a traction splint. In the haemodynamically stable patient with a femoral fracture who is also at risk of pelvic fracture, consideration may be given to the use of one of the varieties of traction splint which does not exert pressure using traction against the pelvis in the midline.
If the patient has significant haemodynamic compromise, in order to prevent delay in transfer to hospital, consideration should be given to pulling the leg(s) out to length (with appropriate analgesia), applying a pelvic splint and then binding the legs together with figure of eight bandages or straps. If attempts to pull the leg out to length appear to worsen the patient's cardiovascular status, immobilisation should be carried out with the legs in the position ‘as found’.
6. Patients should not be log rolled or transported on a spinal board
There is evidence that logrolling patients with significant pelvic fractures can cause clot disruption and further haemodynamic compromise (Lee and Porter, 2007). Patient handling must therefore be approached with care in these patients. Logrolling only has a place in turning a patient onto their back to allow access to their airway. There is no place for routine logrolling in blunt trauma victims. Patients should be moved with the aid of a scoop stretcher. No patient should be logrolled onto or off a spinal board with a pelvic injury.
7. The use of pelvic binders is associated with the risk of low pressure skin necrosis
There is evidence that with a pelvic binder in place, tissue under the binder is at risk of pressure necrosis (Jowett and Bowyer, 2007; Knops et al, 2010; 2011). There are a few case reports in the literature of this complication (Krieg et al, 2005). A study in healthy volunteers demonstrates that the pressure exerted by some of these devices is close to or even over the level capable of compromising tissue perfusion (Knops et al, 2011). In patients with a low blood pressure this is likely to be even more exaggerated. This problem is compounded if the patient is also on a spinal board (Knops et al, 2011).
Using a device that controls the pressure exerted, such as the SAM pelvic sling, might help prevent pressure necrosis, but there is limited clinical evidence to support this recommendation. Providers must be aware of this problem and avoid transporting these patients on spinal boards.
8. The pelvic binder should be placed next to skin
There is limited information regarding this in the literature. Most of the studies have been performed in accident and emergency departments where clothes were removed. Studies examining the effect of pressure exerted by these devices have been undertaken with only thin undergarments on. There is no evidence that placement over clothes provides the same degree of stabilisation or risk of pressure damage. Ideally, pelvic binders should be placed either directly to skin or just over thin underwear. Placement next to skin may allow more accurate positioning of these devices; it will also help prevent the pelvic binder device being removed on arrival at hospital.
In certain scenarios, it may be appropriate to place the binder over clothes and the fear of undressing someone should not prevent the use of these devices.
9. A pelvic binder should be applied prior to extrication
There is no evidence in literature to help guide a recommendation. If early placement controls haemorrhage and movement of an unstable fracture can disrupt clot formation, it would seem logical that placement occurs prior to extrication where possible. This area requires further investigation to find the optimal method for placement of binder. A pragmatic approach is also required as there are likely to be scenarios when placement is not practical prior to extrication.
Conclusion
The consensus statement aims to challenge the view that a pelvic binder is a packaging device. It should be thought of as a treatment option for major haemorrhage.