

A 57-year-old farmer with a medical history of hypertension presented with chest pain. He works as a carpenter and experienced some chest pain yesterday when sawing timber. It radiated down his left arm. He assumed it to be musculoskeleteal pain. The discomfort persisted overnight.
The next morning, he felt his left arm ‘dead’. He went back to work despite feeling unwell. Later that morning, the chest pain increased in intensity and he felt quite nauseous and sweaty. His apprentice drove him to the local emergency department.
His vital signs were as follows:
- Blood pressure: 120/69 mmHg
- Pulse rate: 75 beats per minute
- Respiratory rate: 18 breaths per minute
- Sp02: 94% on air
- Temperature: 37.3°C
The 12-lead electrocardiogram (ECG) in Figure 1 was recorded.
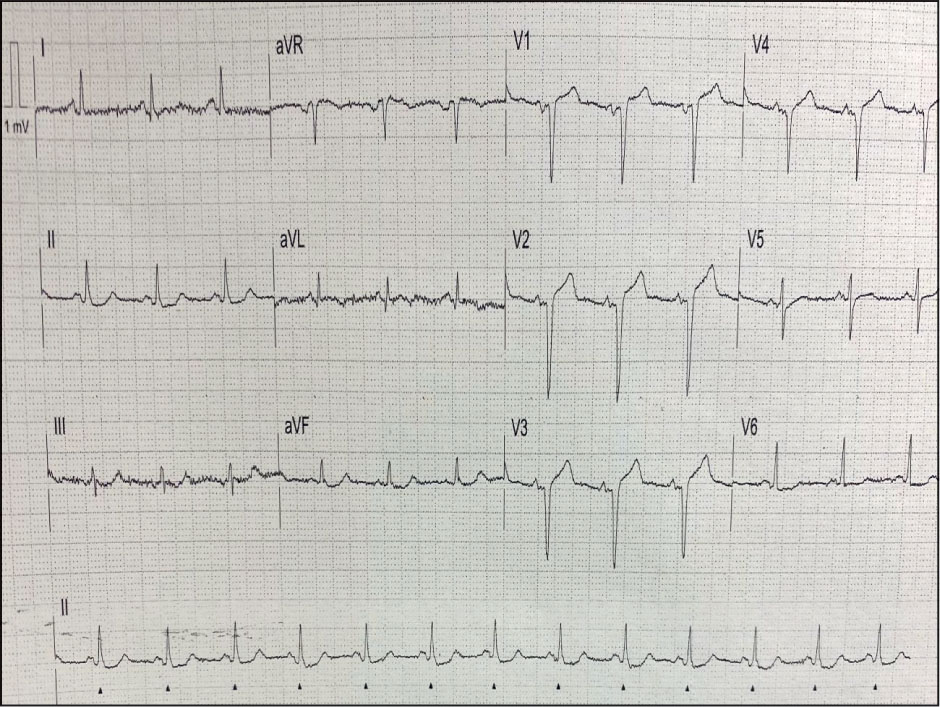
What does the ECG show?
The heart rate is approximately 75 beats per minute and in sinus rhythm. The cardiac axis is normal. There is minimal ST segment elevation in the anterior chest leads V1–V4. There is also deep Q waves in those leads. There is some minor ST segment depression in the inferior leads.
He was triaged to the cardiac catheterisation laboratory for coronary angiography.
His proximal left anterior descending (LAD) coronary artery was completely occluded, with some faint collaterals from the right coronary artery. There was also mild-to-moderate atheroma in the circumflex and right coronary arteries.
A single stent was fitted to the LAD.
Overnight, he was short of breath and became oxygen-dependent. He had crepitations in his lung fields and a chest x-ray showed pulmonary oedema. He was managed with a diuretic and improved. He was discharged home 4 days later.