
Dear Editorial Team,
In your latest issue of the Journal of Paramedic Practice (Volume 10, Issue 9; September 2018), there was an article titled ‘Recognising ECG Landmarks’ written by Karen Simpson-Scott. I would firstly like to state that this was a well written article, and an enjoyable read; however, there are some concerns with the information/images within, that I feel require your urgent attention.
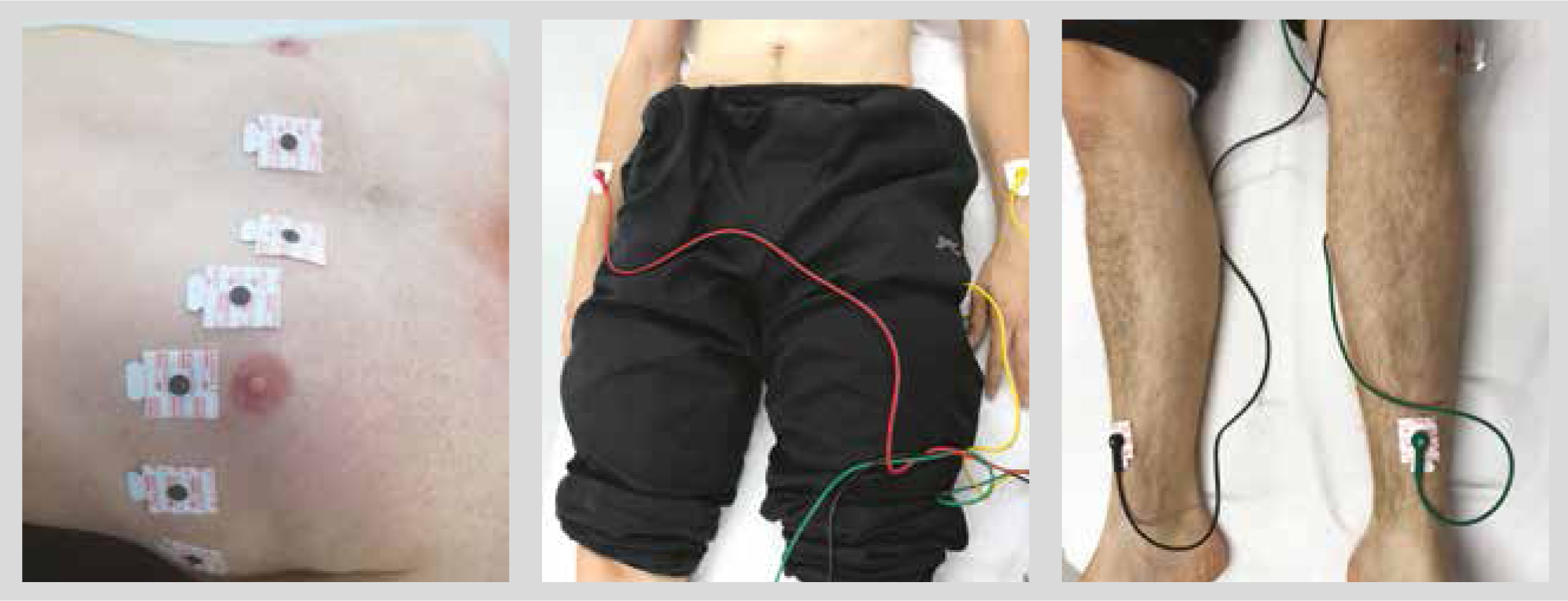
Figure 1, images 1 and 3 show incorrect limb lead/chest lead placements as otherwise correctly described in the article text. Where possible, upper limb leads should be placed proximal to the wrist and, ideally, on a bony prominence. Lower limb leads should be placed proximal to the ankle, again ideally, on a bony prominence. These standardised positions are ‘best practice’ as suggested by the Society for Cardiological Science and Technology (SCST) for obtaining an accurate electrocardiogram (ECG), but also as a standardised approach for serial ECG comparison, which may potentially be between different users and/or settings (i.e. hospital, ambulance, community, practice, etc). Ideally, any variation should be documented on the ECG trace. Image 3 shows incorrect chest lead placement. V1 and V2 are depicted proximal to the 2nd intercostal space, and too far from the border of the sternum. This therefore disrupts all other lead placements. Correct placement images can be found within SCST guidance.
On page 397 in the ‘Chest Lead’ section, there is a sentence that states ‘the third intercostal space should be in line with the angle of louis’. This is incorrect information. The second intercostal space is lateral and slightly inferior to the sternal angle. Once the second intercostal space is palpated, it is then possible to palpate down to the third, and then to the fourth intercostal space. Where the fourth intercostal space meets the sternum, is where V1 and V2 are correctly placed respectively. As already identified in the article text, incorrect chest lead placement can present the clinician with abnormal morphologies, obscuring accurate interpretation of a 12-Lead ECG.
I feel that this information should be reviewed and appropriately communicated in a subsequent issue (or other means) so that best practice for paramedics is continuously promoted, and that the images in this article support and reflect the hard work of the text written within.
Should you require it, here is the link to the SCST Guidance for Recording a Standard 12-Lead Electrocardiogram (issued September 2017) for any further information and/or clarification: http://www.scst.org.uk/resources/SCST_ECG_Recording_Guidelines_20171.pdf
Sincerely yours,
Philip Poskitt
Dear Editor,
I am writing in response to the letter and concerns raised by Mr Philip Poskitt about the recent article I authored titled ‘Recognising ECG Landmarks’. I would like to thank Mr Poskitt for his positive comments about the article and for highlighting his overall concerns. In response to these, indeed it is clear that these two images show incorrect ECG lead placement. Image 1 does not reflect the correct placement as is written in the text. Image 3 also does not represent the correct placement of the chest leads; indeed V1 and V2 are placed too high, disrupting the placement of the subsequent leads. Both images have been updated and sent to the Editorial Team for clarification in the online edition and to accompany this published letter. To produce this article, several images were taken showing both correct placement and also common errors that can occur. Following the initial draft, it was decided not to use the inaccurate images to avoid confusion; however, two of these were sent in error.
Mr Poskitt also correctly highlights the anatomical location of the angle of louis. Within the text, I have stated that it lies in line with the 3rd intercostal space, which is incorrect. The second intercostal space is lateral and slightly inferior to the angle of louis, as clearly seen in image 2. This should then be used to palpate down to the 4th intercostal space at the sternal edge for the placement of V1 and V2.
I would like to thank Mr Poskitt and any other reader who spotted these errors; they were not intentional in their inclusion. Unfortunately, however, these errors are further accentuated by the uncomfortable irony of the title of the article. The purpose of this article was to highlight best practice when recognising ECG landmarks, and it is hoped that the response from readers about this article has created discussion and raised awareness of the importance of correct placement. Thank you once again for your feedback.
Karen Simpson-Scott
CORRECTION TO ARTICLE IN VOLUME 10, ISSUE 9, Journal of Paramedic Practice (p. 396)
Dear Readers,
Further to the letter written to our team by reader, Philip Poskitt, and the accompanying response from author, Karen Simpson-Scott, on p. 236 (opposite), the Journal of Paramedic Practice would like to sincerely apologise for the errors published in the following article:
Simpson-Scott, K. Recognising ECG landmarks. J Para Pract. 2018;10(9):396–398. https://doi.org/10.12968/jpar.2018.10.9.396
The following statement published within the article is
‘The third intercostal space should be in line with the angle of Louis; count this and then locate the fourth intercostal space.’
The correct information has been provided by the author as follows:
The second intercostal space is lateral and slightly inferior to the angle of louis, as clearly seen in image 2.
This should then be used to palpate down to the 4th intercostal space at the sternal edge for the placement of V1 and V2.
Furthermore, the author has provided the below images showing correct ECG placement.
The Journal of Paramedic Practice asks readers to please refrain from following images 1 and 3 from Figure 1 in the above stated article, and rather to use the original article, in conjunction with these letters and this correction, for learning purposes. In the interests of transparency, and open discussion and learning, we will not correct the original article, but will flag up any inaccuracies and signpost readers to these letters and this correction for clarification.
We would like to extend our genuine thanks to Philip Poskitt, and all readers who commented on the article via our social media platforms, for pointing out these errors in the interests of our readership and, ultimately, the patients for whom you care. We would also like to extend our support to Karen Simpson-Scott and the Education team at Edge Hill University.
We want to assure our readers that all articles are peer-reviewed, edited, proofread and approved by the authors prior to publication. However, human error can very occasionally creep in—though we do our best not to let this happen. We are proud to represent the paramedic profession and are committed to continuing to provide a space for the sharing of best practice with the view of supporting the evolution and advancement of paramedics and other providers of pre-hospital care.
Kind regards,
Aysha Mendes