The ‘bugs’ that are commonly caught by people can be more accurately described by the agent that causes the illness. These agents include parasites, fungi, bacteria and viruses. The existence of viruses, taken from the Latin for venom or poison, was suggested at the end of the 19th century but the first virus was not seen, with the aid of an electron microscope, until 1931. A virus is an infectious agent that is totally dependent on its host to provide the means to replicate and thus continue its existence. Without a host, a virus is a simple yet inactive collection of molecules.
Viruses come in a bewildering variety of shapes and sizes, and are spread by a variety of means. The timescale that a virus needs to have an effect on its host can range from the acute to the long– term, and the effect can range from the irritating to the fatal (Hibberts et al. 2004).
The smallpox virus
The smallpox virus (variola major) is a member of the family Poxviridae and the genus orthopoxvirus, which also includes vaccinia and monkeypox. Poxviruses are the largest viruses that cause infection in humans and are complex organisms. Poxviruses can survive and spread in an aerosol form but are killed easily by common detergents (Moore et al. 2006). Smallpox has been responsible for millions of deaths throughout history, an estimated 300 million in the 20th century alone (Crawford, 2000: viii).
Smallpox is highly transmissible, especially between people in close confines. It spreads in an aerosol form containing infected droplets produced in the respiratory tract. Smallpox can be spread by contaminated clothing and bedding (WHO, 2010a) and also direct contact with skin lesions and bodily fluids (Health Protection Agency (HPA), 2008). There is currently no known cure for someone who is infected with this disease and the treatment that can be offered is purely supportive.
Diagnosis and recognition
The signs and symptoms of smallpox develop after an incubation period, where the carrier is not infectious, lasting approximately 12–14 days and include:
Within a few days of these symptoms appearing, the patient will often start to feel better. The symptoms now develop to include the characteristic rash and lesions (WHO, 2010b):
Death from smallpox is caused by toxaemia and often occurs by the 5th day in acute cases (Bossi et al, 2004). Smallpox survivors are often left with characteristic pockmarks on their face and hands. Limb deformities, deafness and blindness have also been reported (Moore et al. 2006; Senior, 2010). Historical figures who survived infection with smallpox include US presidents George Washington and Abraham Lincoln, Beethoven, Elizabeth I and the soviet dictator Stalin (Miravelle and Roos, 2003).
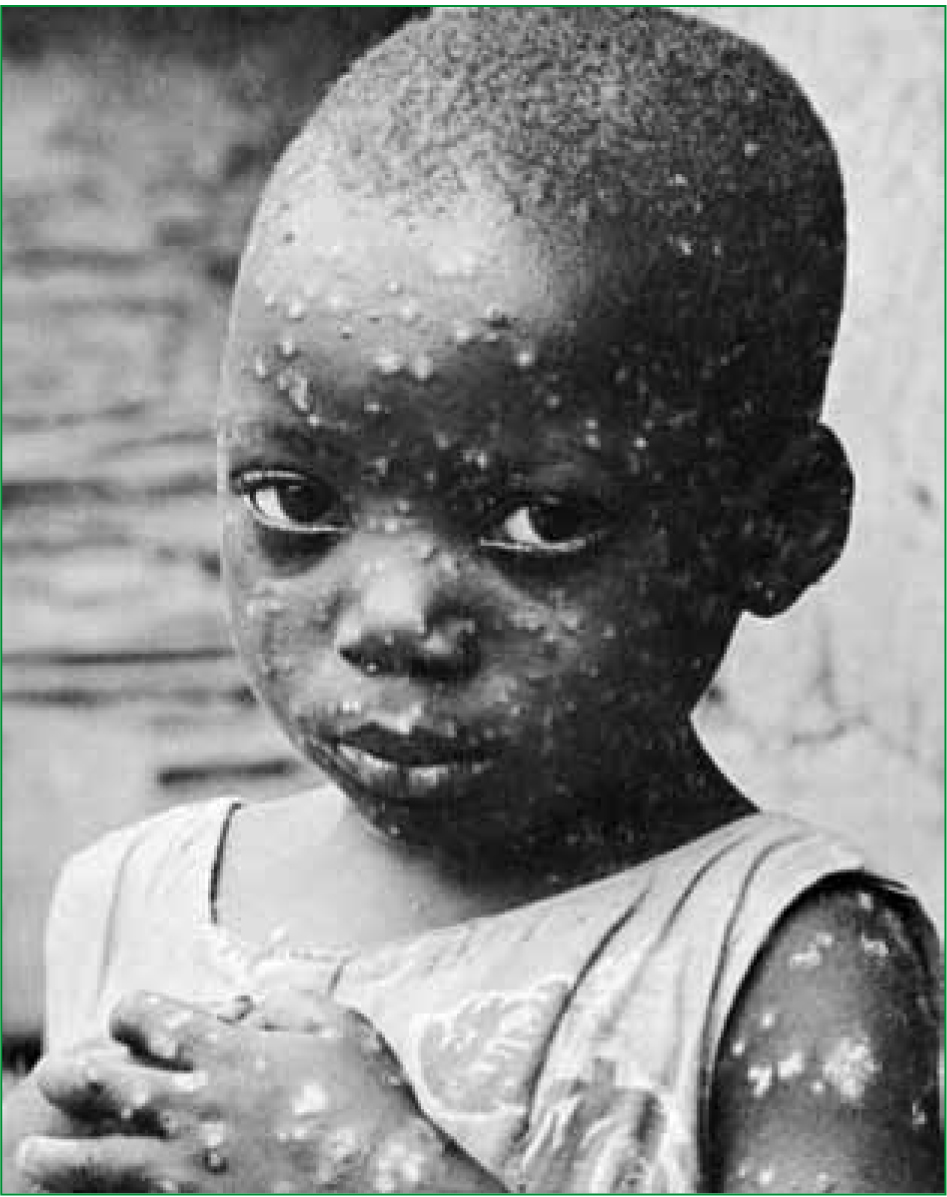
The presentation of smallpox is very similar to the more common chickenpox (Figure 1). The chickenpox rash develops in differing stages, so a sufferer will have pustules at varying stages of development; whereas in smallpox, the pustules are much more uniform in age, often developing over the course of 24 hours. The nature of the rash and the centrifugal spread across the body, concentrating on the face and limbs, including the palms and soles, are characteristic of smallpox (Moore et al. 2006; WHO, 2010a).
There are two recognized forms of smallpox: variola major and variola minor. Variola major is the disease classically known as smallpox which has a mortality rate of approximately 30%. Variola minor is a milder, faster developing form of the infection with a mortality rate of <1% (HPA, 2008). There are also two atypical presentations of smallpox: haemorrhagic and malignant. These atypical presentations occur in a small proportion of sufferers but are fatal in >90% cases.
Haemorrhagic smallpox involves haemorrhage into the mucous membranes and the skin, and presents in a similar fashion to meningococcal septicaemia. Malignant smallpox presented with soft, flat lesions that did develop into pustules (HPA, 2008).
Despite the high fatality rate historically associated with this disease, and the wide geographical spread, this disease is no longer seen by paramedics in the UK or anywhere else in the world, and this is due to vaccination.
Vaccination
Crawford (2000: 202–6) and Stern and Markel (2005) describe how the principles of vaccination were discovered in the 18th century. An English doctor, Edward Jenner (1749-1823), observed that milk maids who were infected with cowpox, a member of the orthopox genus with milder, localized symptoms, seemed to develop immunity to smallpox and did not develop a reaction to variolation.
Variolation was the deliberate introduction of infected material in an attempt to cause a mild smallpox infection which would then leave the person with immunity, if they survived. Jenner demonstrated between 1796 and 1798 that inoculation with cowpox could provide immunity against smallpox. This discovery was revolutionary and laid the foundation of the modern day practice of vaccination (Davey et al. 2003).
Vaccination is the process of sensitising the bodies’ immune response to a particular pathogen by the introduction of a weakened or attenuated version of the infectious agent. The primary immune response is short lived. The secondary immune response when the body meets the live virus is faster and has higher levels of longer lasting antibodies with a greater affinity for the pathogen, therefore a natural resistance occurs and the virus is unable to establish itself (Male, 2007).
Paramedics and vaccination
At present, paramedics in the UK are not routinely involved in vaccination programmes, however this may change in the near future. The College of Paramedics has included administering vaccinations to members of the public as part of the remit for advanced paramedics for, if, or when, paramedic prescribing becomes a reality (College of Paramedics, 2010). This recommendation makes reference to the recent swine flu pandemic and the ability of paramedics to vaccinate members of the public.
Walz et al (2003) published a report examining the use of paramedics to administer vaccinations in the prehospital environment and in the event of a large scale disaster. The report gave a number of examples of paramedic services in the US who are involved in administering vaccination programmes. This report also discusses the training and continuing education needs for paramedics who may be involved in widespread vaccine administration in a bioterrorism event or similar disaster setting. The conclusion of this report is that paramedic administration is a suitable and feasible method for delivering a vaccination programme.
The smallpox vaccine gave immunity against other members of the orthopoxvirus genus such as monkeypox (Moore et al. 2006). Now that the vaccination programme has been stopped, diseases such as monkeypox are on the rise in countries such as the Democratic Republic of Congo (Peeples, 2010). Smallpox does not appear to be zoonotic, like its cousin monkeypox, meaning that it appears to have no animal reservoir in the natural environment.
The lack of an animal reservoir was one of the factors that enabled this disease to be eradicated as treatment measures could be directed at the human population without considering if there was an unknown carrier still waiting to be discovered.
Risks from vaccination
The process of vaccination does unfortunately have some risks. The smallpox vaccine uses live virus and when used in the 1960s caused 1–3 deaths per million doses (Davey et al. 2003: 72). The lack of any immunization since the 1970s may cause an increased mortality rate if the vaccine is used in modern times. People being vaccinated for the first time are more likely to develop side–effects than people who have been previously exposed to the virus.
In this age of modern medicine, there are more immunosuppressed individuals and people who would be at higher risk of side–effects from the vaccine than in previous times. A subject who has been exposed to smallpox can be vaccinated as a precautionary and prophylactic measure. If vaccination is administered with 4 days of exposure the mortality can be reduced by 50% (Miravelle and Roos, 2003; HPA, 2008).
There are differing methods of vaccinating a population in the case of the release of an infectious agent such as smallpox. There are arguments for two proposed solutions, one being mass vaccination (MV) and the other being targeted vaccination (TV). MV involves vaccinating as much of the population that is susceptible as soon as possible in order to raise the general level of immunity and starve the virus of potential hosts.
TV involves tracing and vaccinating exposed and at risk individuals in a bid to contain an outbreak. Kaplan et al (2002) put forward the case for mass vaccination outperforming targeted vaccination in the event of a smallpox outbreak. The current policy of the Department of Health (DH) is TV followed by a plan to escalate to MV if necessary (DH, 2003).
The current situation
Today smallpox is no longer considered a naturally occurring threat and many people will know little or nothing about this disease that was once a plague on mankind. In 1966, the WHO initiated a programme designed to eradicate smallpox. This programme was declared successful in 1980 and is the only example of a human disease being wiped out by human intervention as of this writing.
The last recorded fatality caused by smallpox was in the UK in 1978. The victim was a photographer working at the University of Birmingham medical school who caught the virus when it was not safely contained in the microbiology department on the floor below where she worked (Crawford, 2000).
The UN recently announced the eradication of a second viral disease, this time a disease that affects cattle called rinderpest. This shows that vaccination programmes have applications outside of human medicine (WHO, 1980; Ghosh, 2010).
There are still legally held stockpiles of the smallpox virus known to be kept at the Centre for Disease Control and Prevention (CDC) in the US and at the State Research Centre for Virology and Biotechnology (VECTOR) in Russia (Moore et al. 2006). These viruses are kept under the highest security and have been the subject of much discussion and controversy. Whether there are stocks of the virus elsewhere is unknown, but this possibility is of great concern. Nobel prize winner Joshua Lederberg states in no uncertain terms ‘The single biggest threat to man’s continued dominance on the planet is a virus.’ (Crawford, 2000).
Smallpox may have been eradicated in the wild but, with the technology that is available today, people may be able to recreate this ancient scourge. In 2006, The Guardian newspaper ordered a segment of smallpox DNA and had it delivered to a made-up company to illustrate the ease with which this could be acquired (Randerson, 2006). Baker (2010) and McFadden (2010) both describe concerns that in this age of DNA gene synthesis, the re-emergence of smallpox from a laboratory created source is possible.
Now that the vaccination programme has been ceased, and the disease is no longer present in the general population, the level of background immunity to this virus will fall as time passes. This lowering of our natural immunity may mean that any new outbreak, whether from an unsuspected natural source or a deliberate release, may spread rapidly and have dire consequences.
In 2005, it was reported that the UK had enough vaccine to vaccinate the entire population. Other European countries have similar stockpiles. The Netherlands has enough vaccine to vaccinate its entire population and has plans to enable this to be done within 4 days (Arita, 2005). Currently there are 300 million doses of vaccine stockpiled in the US compared to only 12 million doses available for a population of 280 million in 2001 (Sternberg, 2010). This rapid increase is a reflection of the seriousness with which this threat is being taken and is one more effect that could be attributed to the 9/11 attacks.
In the current climate where the threat of a terrorist attack is never far from the news and where there have been examples of the use of chemical and biological weapons in recent history, one of the major threats is the release of the smallpox virus (Atlas, 2002). Various forms of spreading disease, pre-dating the discovery of bacteria and viruses, have been used in warfare since ancient times. One of the first recorded incidences of the deliberate use of the smallpox virus in warfare involved the British forces giving contaminated blankets to the native Americans who were attacking settlers in the new world in 1763 (Crawford, 2000).
‘In the event of an outbreak, paramedics may well encounter the ‘worried well’ who believe they have been exposed to the virus or who are worried about symptoms of similar conditions’
To destroy or not to destroy? That is the question
In light of the threat posed by the smallpox virus, there has been heated debate over what should be done with these remaining stocks. Do we have the right to destroy any organism, wilfully and in full understanding of what we do? Should stock be kept for research purposes and for producing a vaccine should a natural outbreak ever appear?
Is keeping a virus as deadly as smallpox a mistake that may one day come back to wreak havoc on a population who have no immunity to it?
The WHO originally directed that all stocks of smallpox be destroyed when eradication was confirmed, but this final act has been continually delayed. The reasons cited for maintaining these stocks are research related. The latest debate on the subject of destroying the remaining stocks was held at a symposium in Brazil in August this year. In 2011, the WHO will review ongoing research and once again debate the fate of the remaining smallpox (Senior, 2010).
There are now a group of diseases that are classified as vaccine-preventable diseases (VPDs). This group includes diphtheria, hepatitis B, measles, polio and tuberculosis (WHO, 2010c). Efforts are being made to pursue eradication campaigns against some of these diseases, using vaccination in a similar manner to smallpox (The Global Polio Eradication Initiative, 2010). The burden of many of these VPDs falls on developing countries where the finances for healthcare and vaccination programmes are not available.
Why smallpox matter to paramedics
Some people may question how relevant knowledge of a disease, that we should never encounter, may be to a paramedic who has many other facts, figures, procedures and protocols to learn, remember and apply. As paramedics working in the widely varying field that is our prehospital workplace, one of the first lessons that we all learn is scene safety. We learn to protect ourselves by the use of gloves, barriers, aseptic techniques and conflict resolution courses. How much consideration do we give to the protection provided by the various vaccinations that we have all had, not just as paramedics, but as children and as we go through our lives?
If there was an outbreak of smallpox, it would be up to physicians and medical personnel to spot this at the earliest possible opportunity to stop a rapid and wide spread. Madeley (2003) states that the speed with which an accurate diagnosis can be made will be critical.
The similarities between the presentation of smallpox and diseases such as chickenpox, along with the lack of familiarity, and the fact that most people consider this disease extinct, could easily allow a covert outbreak to spread rapidly.
Paramedics, along with other prehospital care providers and frontline medical staff, would be at high risk of exposure.
Mackler, Wilkerson and Cinti (2007) published results of a study into whether paramedics would report for work in the case of a pandemic. Depending on the level of protection provided to the paramedics, both by vaccination and protective equipment, up to 80% said they would not remain on duty if they were not adequately protected. Even when protection is provided to the paramedics, the level of protection of family members had a large impact on the numbers who would report for duty. The conclusion of this survey was that first responders must be protected and educated regarding pandemics.
The recent swine flu and bird flu episodes and the resulting panic, highlights the effect that an easily transmissible and well publicised disease can have on the general public (Bonneux and Van Damme, 2006; Fitzpatrick, 2009). If there was a deliberate release of an infectious agent, the likely result would be mass panic and demand for vaccination (Kaplan et al. 2002). The number of calls received by the emergency services, and the response we are called upon to provide, would likely be overwhelming.
In 2002, a survey was conducted in America to gauge the level of knowledge held by the public regarding smallpox. This survey was conducted when smallpox had been raised in the public’s awareness by a recent announcement by the Bush administration that troops heading to Iraq, emergency personnel and health care staff were to be vaccinated against smallpox due to a perceived threat. Blendon et al (2003) found that the public were ill–informed and had little knowledge of this disease, highlighting the fact that the medical community would have an educating role to play if such an event occurred.
In this age of twenty–four hour news and the worldwide web, information is easily accessible. However, just because information is available does not mean that it is accurate or easy to understand. If smallpox were mentioned in the media in connection with either a natural outbreak or a deliberate release, the information people could access may add to the panic or it may reassure people. The message conveyed by the press would be crucial in how the public would react to such an event.
As paramedics, we can provide accurate and reassuring information to hopefully calm and educate our patients if we have good background knowledge of these agents.
Medical staff would not normally be called upon to enter an exposed zone if there was a confirmed, or suspected, release of smallpox due to the high risk of infection by inhalation. The HPA (2008) recommends protective clothing including a respirator and a biologically-resistant suit for such a task. In recent years in the UK, paramedics working within the Hazardous Area Response Teams (HART) have been provided with, and trained in the use of protective equipment that would allow them to work alongside the HPA and other agencies and assess and treat patients in the event of a biological agent such as smallpox being released (HART, 2010).
Conclusion
Smallpox was once a global killer but was eradicated by a concerted and prolonged global effort. The development of vaccination and its widespread adoption has undoubtedly saved millions of lives around the world. In the future, vaccination may be the key to consigning further diseases to the history books. The threat of a re-emergence, either from a natural source or from a strain created in a laboratory, means we cannot forget about smallpox.
In the future, a disease may emerge similar to smallpox. An understanding of what resources are in place to deal with various infectious disease outbreaks may prove useful. Paramedics can continue to rely on protection from vaccines in the same manner as the general public and may be involved in administering vaccination programmes in the future.