
Apreviously fit and healthy 35-year-old man presented with a seizure. He was out shopping when he felt cold, clammy and faint. He sat down but was then helped to the floor as he became unresponsive. He was vacant for approximately 1–2 minutes with twitching of his legs. There had been no preceding prodromal symptoms such as palpitation. When the paramedics arrived 5 minutes later, he was drowsy but responsive, and complaining of frontal headache. His vital signs were:
He was taken to the emergency department. A subsequent computerised tomography (CT) scan showed no abnormality within his brain. A 12-lead ECG was recorded.
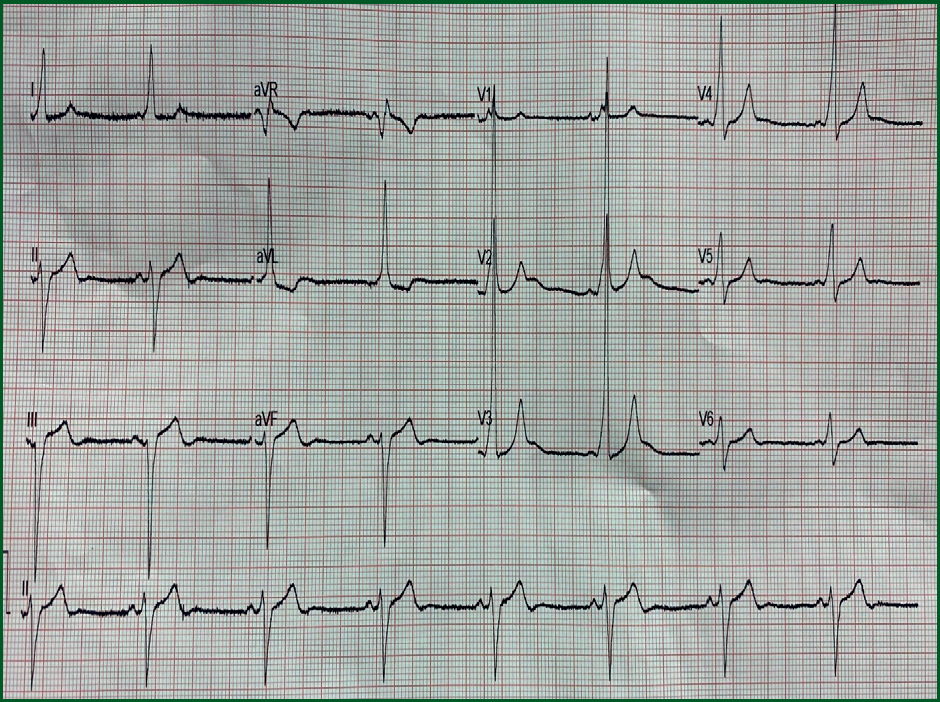
What does the ECG show?
The heart rate is approximately 50 beats per minute and in sinus rhythm. There is left axis deviation.
The ECG shows some significant abnormalities:
These ECG appearances are in keeping with a diagnosis of Wolff Parkinson White (WPW) syndrome. This condition is often associated with cardiac tachyarrhythmias that are usually atrial in origin. Whether or not an arrhythmia was responsible for his seizure is unclear.
In normal individuals, electrical activity in the heart is initiated in the sinoatrial (SA) node, propagates to the atrioventricular (AV) node, and then through to the ventricles. The AV node acts as a gatekeeper, limiting the electrical activity that reaches the ventricles of the heart. Individuals with WPW syndrome have an accessory pathway that connects the atria and the ventricles, in addition to the AV node. This accessory pathway is known as the Bundle of Kent. This accessory pathway does not share the rate-slowing properties of the AV node, and may conduct electrical activity at a significantly higher rate than the AV node.
The accessory pathway results in early electrical activation of one ventricle (pre-excitation) There is a predisposition to atrial tachyarrhythmias.
An implantable loop recorder was inserted in this man to determine whether he was experiencing arrhythmias and, if so, whether they were associated with syncopal episodes.