


While penetrating wounds caused by frearms or explosions are mercifully rare within the UK civilian pre-hospital environment, the provision of optimum care is likely to depend upon emergency responders having an appreciation of the unique nature of such injuries. Understanding some of the basic elements of ballistic injury is also an important factor in determining the potential damage caused by different kinds of frearms and propellants. During 2009–2010, recorded frearms offences involved 2,115 injuries (including 40 fatalities) caused by the discharging of a variety of weapons, a majority of which were inficted by handguns, athough shotguns, rifes and air weapons also featured (Eder, 2011). For each of these different weapon types, a specifc wound profle will have been produced, the pattern that will have been determined by the occurring circumstances, and nature of the tissues involved.
The science of wound ballistics incorporates the interaction between human tissues and projectiles such as ‘bullets and fragments from explosive weapons’, and is a feld in which many healthcare professionals have only limited experience (Mahoney et al, 2005; ICRC, 2008). Even though the study and analysis of wound ballistics is ostensibly based upon objective physical properties, there has also been considerable controversy suggested by the relevent literature that many authors consider to be misleading for those responsible in managing such injuries (Fackler, 1987; Ryan et al, 1997). In order to understand the mechanisms and patterns of injury associated with wound ballistics, and to make sense of any potentially conficting guidance on the subject, it will be helpful to obtain a basic knowledge of how kinetic energy is transferred from the projectile to tissues within the body, and the resulting risk of damage to them, as well as the location of the injury upon the body and the velocity, mass and fight characteristics of the penetrating projectile.
The relationship between kinetic energy and the potential to cause injury
The capacity for a penetrating projectile to cause damage to tissues is determined by its kinetic perform work’, like any form of energy, is subject to the law of energy conservation, which dictates that energy itself is not created or destroyed merely altered to a different state. Under these circumstances, once penetration has occurred the kinetic energy of a projectile is effectively converted into a form which may lacerate and crush tissues directly along the wound track and that can potentially damage radial structures through cavitation (Ryan et al, 1997; Beiser 2003).
The kinetic energy of a projectile (and as an extension, its destructive potential) can be calculated using the following formula:
kinetic energy =1/2 Mass x velocity2
This formula clearly indicates that an incremental increase in velocity (squared) will have a far greater effect than mass (halved) upon the generation of kinetic energy. Therefore, if taken in isolation, this formula would suggest that the velocity of a penetrating projectile will be a much greater determinant of potential injury (Coupland et al, 2000). However, basing the wounding potential of a penetrating projectile primarily upon a formula for calculating kinetic energy (with an explicit emphasis upon velocity) has been the subject of controversy and misinterpretation within relevent medical literature (Ryan et al, 1997). Dividing wounds into ‘high’ and ‘low’ velocity catagories, depending upon how the projectile was propelled or the type of weapon involved, is also considered to be counterproductive with regards to assessment and surgical intervention (Fackler, 1987).
A more commonly accepted approach to classifying ballistic wounds is to consider the means by which the kinetic energy is actually dissipated to the affected tissues, with associated injuries classifed as either ‘low or high-energy-transfer’ (Ryan et al,1997; Clasper, 2001). However, considering the wounding potential of a projectile solely in terms of kinetic energy transfer can discount several key interactions that occur between the tissue and projectile. These interactions incorporate the dissipation of kinetic energy (with reduced injury potential) through the generation of heat, radial tissue movement, projectile deformation and the creation of a sonic pressure wave. While a penetrating projectile will inevitably lacerate and crush structures directly in its path, it is often overlooked that many living tissues have a high tolerance to injuries associated with the stretching and shearing forces of ‘high-velocity’ energy transference (Fackler, 1987; Ryan et al, 1997).
The consequences of energy transfer: direct injury, cavitation and pressure waves
‘Health professionals, who treat people wounded by weapons, will beneft from a better understanding of the physical process of wounding’ (ICRC, 2008)
Once the tensile resistance of the skin has been overcome, penetrating projectiles will cause injury through direct laceration and compression. The permanent cavity formed by this mechanism of damage follows the path of penetration, and is proportional to the size and surface area of the projectile directly in contact with the tissues (Jenkins, 2005). In addition to the permanent cavity, higher levels of kinetic energy transference cause the formation of a temporary cavity through the radial acceleration of tissues away from the path of the projectile shortly after it passage (Ryan et al, 1997). The resulting temporary cavity will usually last for between 10–30 milliseconds and reach a maximum volume (potentially 10–40 times larger than the projectile diameter) within 1–4 milliseconds of impact. After a brief period of oscillation the cavity will then collapse, generating an area of sub-atmospheric pressure that can draw potential contaminants deep into the wound (Clasper, 2001; Stapley 2007).
Although the clinical consequences of temporary cavitation have been the subject of misinterpretation and controversy in the past (Fackler, 1987; Ryan et al, 1997), it is the capacity for damage to tissues beyond the permanent wound track that is of key importance. Under these circumstances, the radial stretching and shearing forces, also known as the zone of ‘contusion’, may extend for several centimetres away from the wound track, causing micro-vascular disruption and devitalisation (Coupland, 2001; Hill, 2001; Goonewardine, 2007). This damage can also be distributed asymmetrically as energy is channelled along fascial planes and into structures which are more remote from the immediate site of injury (Stapley, 2007). Though the creation of this temporary cavity is infuenced by projectile velocity and the transference of kinetic energy, the size of the projectile and its potential to cause injury is also dependent upon the behaviour of the projectile after penetration, as well as the composition of disrupted tissues (Coupland, 2000; Clasper, 2001; Jenkins, 2005).
In addition to the disruption associated with permanent and temporary cavitation, the creation of a sonic pressure wave represents an additional form of potential injury, though this remains an issue of some dispute. The transmission of a pressure wave occurs in the wake of a projectile moving faster than the speed of sound through air. As tissues convey pressure waves much more effciently than air, the rate of transmission is increased once the projectile begins to move through the body, causing the pressure wave to precede the projectile (Fackler, 1987). Although regarded by some prominent authors as an irrelevnt phenomenon (Fackler 1987; Ryan et al, 1997: 39), a literature review (Courtney and Courtney, 2007) revealed that the pressure wave generated by a high velocity projectile can be suffcient to cause mild to moderate traumatic brain injury, and it has been suggested that the resultant ‘concussive-like’ effects are most likely to cause acute neurological incapacitation, with potential of long-term sequelae in approximately half of all patients who have received a thoracic gunshot wound generating a pressure wave in excess of 1000 psi. This this would, however, exclude many lower velocity frearms from such an effect.
The nature and composition of the projectile
‘The shape and material composition of the projectiles have a stronger infuence on destruction than velocity’ (von See, 2009)
Despite the promenent role of velocity in determining the potential of kinetic energy generated, the nature of the projectile and its behaviour within living tissues remain the major determinants of how and when that energy is dissipated. Within the civilian pre-hospital environment, such wounds may also be caused by a myriad of purpose-made, improvised or unintended projectiles, each of which will have a unique profle and distribution of mass.
Even purpose-made projectiles such as bullets can differ greatly in terms of their size, shape and composition. Since the Hague Declaration of 1899 (prohibiting the use of bullets designed to expand or fatten on impact), virtually all military bullets used by signatory nations are required to be encased in hard copper shells, or full metal jackets (FMJ) which only permit a small section of the lead core to be exposed at the base. There remain some exceptions to this rule however, including the ‘ballistic hollow point’ bullet, used by some specialised sniper units (Mast and Halberstadt, 2007). In contrast to this, civilian semi-Jacketed (SJ) and hollow point bullets, designed to fatten and deform on impact, have their more malleable core exposed at the tip and are only partially encased within a copper-nickel alloy shell (ICRC, 2008; von See, 2009). In general terms, military bullets fred from higher-velocity (900 m/s) weapons tend to be narrower, more sharply tapered, and have less mass than the shorter and blunter lower-velocity (200-300 m/s) bullets fred by handguns (Ryan et al, 1997).
Fragments from an explosion can originate directly from the device casing (known as primary fragments) or may otherwise be generated by the surrounding environment (known as secondary fragments), in either case however, there is likely to be a great variance in their mass, shape and composition, as well as their wounding potential which will be infuenced by unpredictable impact velocities and differences in the size or angle of the projectile. Additionally, projectiles fred from a shotgun may also vary considerably in size, mass and velocity, depending upon the kind of ammunition used and the gauge of the weapon. Shotgun projectiles may consist of multiple lead, alloy, jacketed or steel pellets or ‘shot’, or alternatively, one large malleable ‘slug’, comparable to an outsized unjacketed handgun bullet (Ryan et al, 1997).
Deviation from the line of fight, deformation and fragmentation
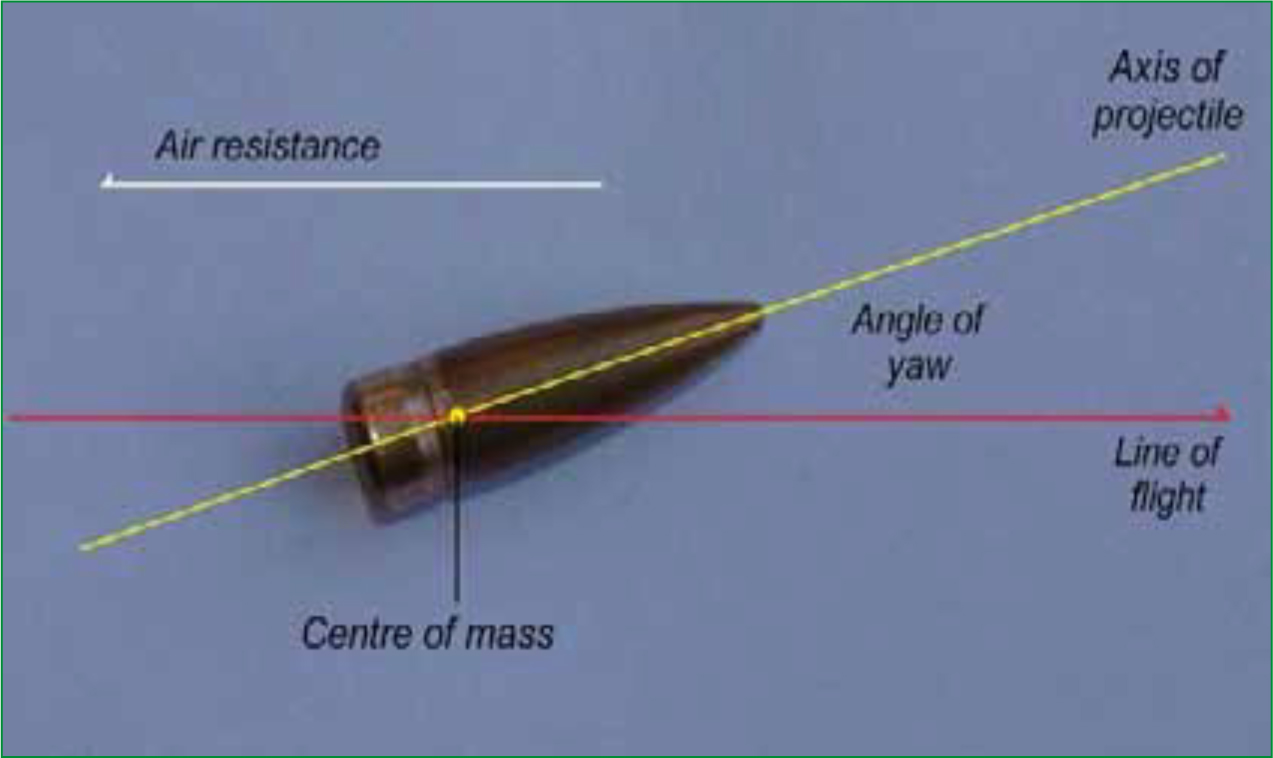
The amount of kinetic energy transferred to tissues from the passage of a penetrating projectile is signifcantly infuenced by its presented surface area, and whether deformation and/or fragmentation of the projectile occurs. In the case of a bullet, the area of presentation is dictated by the degree of yaw, or ‘tumble’ that the bullet experiances in fight, resulting in deviation from the line of aerodynamic tajectory, thereby exposing a larger surface area of the bullet to the affected tissues (Vallema and Scholtz, 2005). Although bullets are inherently asymmetric and often have their centre of mass offset to the rear (making them fundamentally unstable in fight) their potential to yaw is reduced by a longitudinal rotation imparted by spiral grooves, also known as rifing, cut into the barrels of all rifes and some modern handguns (Hollerman, 1990; Ryan et al, 1997). Even with this rotational spin however, this stabilizing infuence does not take full effect for some distance into the fight of the bullet, meaning that yawing (which may be between 2–6 ?) is likely to be much more pronounced when bullets are fred into tissues from a closer range (Ryan et al, 1997, Stapley 2006).
Despite the stabilization imparted by the effect of rifing, the longitudinal rotation of the bullet will eventually be overwhelmed when the bullet enters the denser medium of human tissue, and whatever degree of yaw that remains at that time will be exaggerated as a result. Ultimately, this process will continue to increase until the bullet completely ‘tumbles’ 180 °, and its centre of mass is situated at the forefront of it’s trajectory. If this process takes place in tissues of uniform density then maximum retardation and energy transference will occur when the bullet is at 90 °, travelling sideways to its line of trajectory (Ryan et al, 1997; Hollerman, 1990). Following penetration, bullets with lower inherent stability such as those with less mass, are liable to ‘tumble’ more rapidly, resulting in the transference of large amounts of kinetic energy at a much earlier point along the wound track (Ryan et al, 1997; ICRC, 2008). Similarly, larger, irregularly shaped primary and secondary fragments travelling at higher velocities are also liable to cause greater amounts of tissue disruption, with associated temporary cavitation close to the point of penetration (Ryan et al, 1997).
Higher rates of energy transference and retardation also increase the likelihood that the projectile will disintegrate. When higher velocities are involved, such fragmentation may cause large amounts of tissue disruption from the creation of secondary projectiles and through multiple laceration of surrounding muscular bundles, render them less capable of absorbing the stretching and shearing forces associated with temporary cavitation (Fackler, 1984; Valema and Scholtz, 2005). This phenomenon is applicable to most penetrating projectiles, and is even associated with FMJ bullets which, despite being specifcally designed to maintain their integrity, have been known to fragment when ‘tumbling’ at high velocity through certain tissues (Ryan et al, 1997).
In contrast, unjacketed SJ bullets including hollow-point and illegally ‘modifed’ FMJ bullets, are actually designed to fragment and deform shortly after penetration. Although the ‘mushrooming’ effect of gross deformation is likely to prevent the ‘tumbling’ phenomena more commonly associated with tapered high-velocity FMJ bullets, the increase in frontal surface area acts in causing signifcant retardation and energy transference (Hollerman, 1990; Vellema and Scholtz, 2005). Such projectiles are prohibited in warfare, partially because of the signifcant and debilitating injury they are likely to cause, but primarily due to the energy transference and disruption they can impart at an early stage along the wound track (Coupland, 2000; von See, 2009). Transferring large amounts of energy at an earlier stage means that the projectile is less likely to exit the victim taking kinetic energy with it, but also ensures that a shorter wound track, such as the passage through a limb, will result in far more devastating injuries to the victim. SJ bullets are predominantly used for ensuring a quick kill during hunting and for law enforcement, where having the bullet remain within the victim is likely to reduce collateral damage and injury (Hollerman, 1990; Clasper, 2001; von See, 2009). However, such wounds can still be encountered within the civilian pre-hospital environment, owing to the potential for accidents to occur on hunting trips and fring ranges, and also due to the unregulated nature of illegally owned or obtained frearms.
Density and quality of affected tissues
The kinetic energy deposited along the wound track is dependent upon such factors as mass, velocity and fragmentation, as well as any variances in presented area caused by the yaw and deformation of the projectile. It is wrong to assume, however, that because kinetic energy may be deposited in a particular manner by the projectile, the same level of disruption will occur in each instance. Specifc tissue density and its tolerance to stretching and shearing, play a signifcant part in the mediation of temporary cavitation and displacement.
Tissues with greater density will cause increased retardation, and, in the case of a bullet, are likely to increase the risk of ‘tumbling’. Denser tissues with minimal elasticity and/or encased within connective fascia or bone, such as the liver, spleen and brain, are also unable to expand under the pressure of the temporary cavity and are therefore liable to undergo potentially catastrophic levels of disruption (Vellema and Scholtz, 2005, Ryan et al, 1997). If the projectile strikes bone then signifcant retardation, deformation and fragmentation is likely to occur, amid various degrees of fracture, with the potnetial for additional damage to be cuased by shards of bone acting as internal ‘secondary missiles’ (Hollerman, 1990; Ryan, 1997; Hill, 2001). Tissues with lesser density and/or higher levels of elasticity however, such as the lungs, bowels, and muscular tissue, are more capable of withstanding temporary high energy displacement, and tend to endure with much less permanent damage (Vellema and Scholtz, 2005; Fackler, 1987; Goonewardene et al, 2007).
The length of the wound track also plays a considerable part in determining the potential level of energy transferred by the projectile to surrounding tissue, and a high velocity FMJ bullet, which does not yaw signifcantly or fragment, can pass completely though the muscular tissue of a limb taking much of its kinetic energy with it. A longer wound track however, such as those involved in abdominal penetration, is more likely to give the same FMJ bullet greater opportunity to ‘tumble’ and/or fragment, thereby imparting far more energy to the surrounding structures (Hollerman, 1990; Ryan et al, 1997; Clasper, 2001). The capacity for SJ bullets and other malleable or fragmenting projectiles to deliver larger amounts of kinetic energy near their point of entry, thereby imparting far more disruption along a shorter wound track is the main reason for their prohibition within armed confict (Coupland, 2000).
Entrance and exit wounds
As part of the assessment for penetrating projectile injury it is generally recommended that pre-hospital care practitioners search for and evaluate both entrance and exit wounds (PHTLS, 2007). The mere presence of an exit wound does at least suggest that some kinetic energy has exited the body along with the projectile, however, while the changing characteristics of a projectile within tissues generally ensures that exit wounds are larger and more irregular than entrance wounds, there is no guarantee that such a predictable pattern will always occur, and it is clinically unsafe to draw conclusions about the level of potential injury caused based solely upon these indicators (Ryan et al, 1997; Vellema and Scholtz, 2005).
Bomb fragments and bullets which have become unstable or that ricochet during fight may not strike with their smallest profle area and are likely to cause an entrance wound that is large and irregular. In addition, such projectiles travelling at high velocity, can worsen the desruption at the point of entry due to the energy transference and cavitation that is likely to occur shortly after impact. Under these circumstances, with much of the kinetic energy dissipated during the passage though the body, the exit wound, if present, is likely to be much smaller than the entrance wound. Similarly, relatively small entrance and exit wounds do not always suggest that minimal tissue disruption has taken place, as in the case of a longer wound track, a bullet can leave an unremarkable entrance wound, cause a large amount of disruption deep within the tissues, and fnally leave the body with much of its energy spent through a relatively small exit wound (Fackler, 1987; Ryan et al, 1997).
To add further complexity to the issue, the passage of a projectile through tissues may not necessarily bear a close relationship to the location of any existing entrance and exit wounds, due to potential for defection or internal richochet to occur, most likely to be caused by dense internal structures such as bone. The result of this can be misleading, as any actual internal injury caused by the projectile may be very different to that which the pre-hospital care practitioner may assume to have been caused by a ‘through and through’ wound track. For example, a bullet striking the right anterior chest wall may be defected around the thoracic cavity by the curvature of a rib and exiting through the paravertebral tissues of the back, thereby avoiding vital thoracic structures (Barker, 2001).
Conclusion
For pre-hospital emergency care providers, a basic appreciation of how penetrating projectiles interact with tissues can make signifcant difference to the initial priorities of treatment and transportation. Different projectiles propelled at varying velocities and under different circumstances will produce a variety of wound profles, and the anatomical region which is struck, will also play a major part in the behaviour of the projectile and the degree of tissue disruption sustained.
Determining wound severity purely on the basis of projectile velocity is likely to be clinically unsafe, as can overreliance upon the location and appearance of entrance and exit wounds. However, understanding some of the fundamentals of wound ballistics; especially the manner of kinetic energy transference, projectile behaviour and the tolerances of different tissues may help emergency care providers to make informed decisions when presented with penetrating projectile injuries.