
This 32-year-old lady normally keeps fit and well. She delivered a healthy baby boy by caesarean section 10 days ago following an uncomplicated pregnancy. She has maintained good health throughout her life.
This morning while breastfeeding her baby, she felt acutely unwell. She felt a tightening pressure developing within her chest over several minutes. She was very sweaty and frightened. Her husband immediately called for an ambulance. The ECG in Figure 1 was taken.
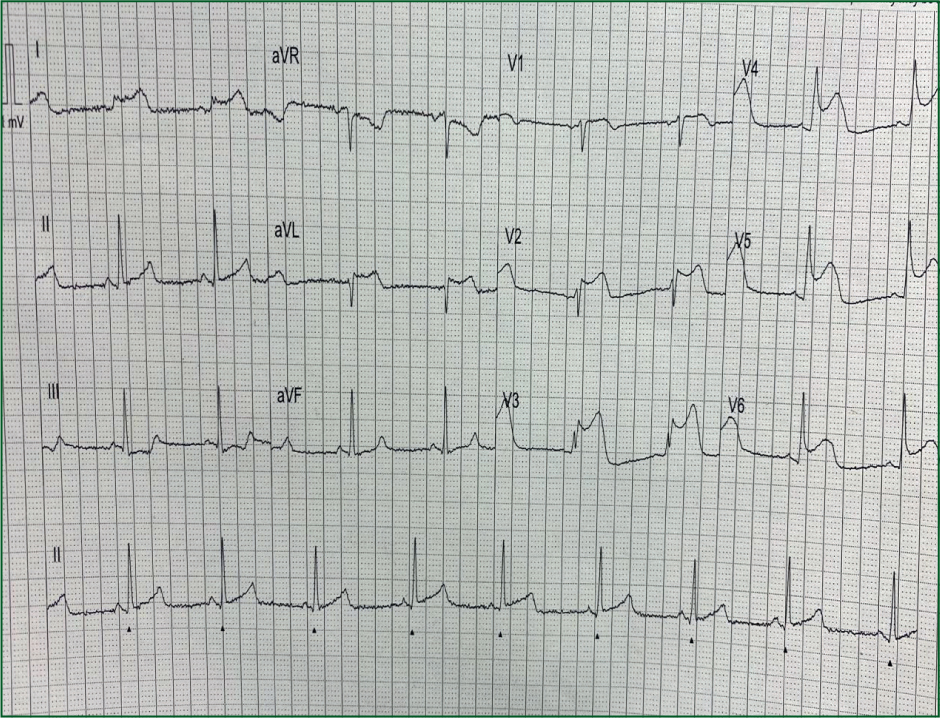
What does the ECG show?
Interpretation of the ECG rhythm
Interpretation of the 12-lead ECG
She was triaged to the catheterisation laboratory for emergency primary percutaneous coronary intervention.
The diagnosis at coronary angiography was of spontaneous coronary artery dissection (SCAD) of the proximal left anterior descending coronary artery.
SCAD is an uncommon non-atherosclerotic cause of heart attack. Rupture of the intimal layer of the coronary artery allows blood between the middle and inner layers resulting in the development of haematoma within the tunica media, leading to separation of the intima. Haematoma from the false lumen that is formed compresses the true lumen and restricts blood flow.
SCAD can affect anyone. However, approximately 90% are female with a mean age in the mid 40s. Affected patients invariably have few conventional risk factors for coronary heart disease.
SCAD is the commonest cause of pregnancy-associated myocardial infarction with almost two-thirds of cases occurring 1-week post partum (it affects 1.81 per 100 000 pregnancies). Pregnancy-related SCAD cases are generally more severe than non-pregnant cases.
As in this particular case, clinical presentation can be similar to atherosclerotic acute coronary syndrome cases. The majority of patients experience ischaemic chest pain. Non-ST segment elevation myocardial infarction (NSTEMI) is the commonest presentation although STEMI, arrhythmias and sudden cardiac death may also occur.
The primary means of diagnosing SCAD is coronary angiography. The left anterior descending coronary artery is most commonly affected, hence anterior (V1–V4). ECG changes are seen in most cases.