
This 52-year-old lady normally keeps fit and well. She has had hypertension for 15 years but this is usually well controlled.
She has been experiencing a lot of stress at home lately, having just separated from her husband. Her son was also badly injured in a road traffic accident 2 weeks ago.
This morning, she was awakened with heavy, central chest pain that radiated down both upper arms and into her jaws. She felt clammy and neaseous. Her daughter immediately called 999.
The 12-lead ECG pictured in Figure 1 was recorded at the scene.
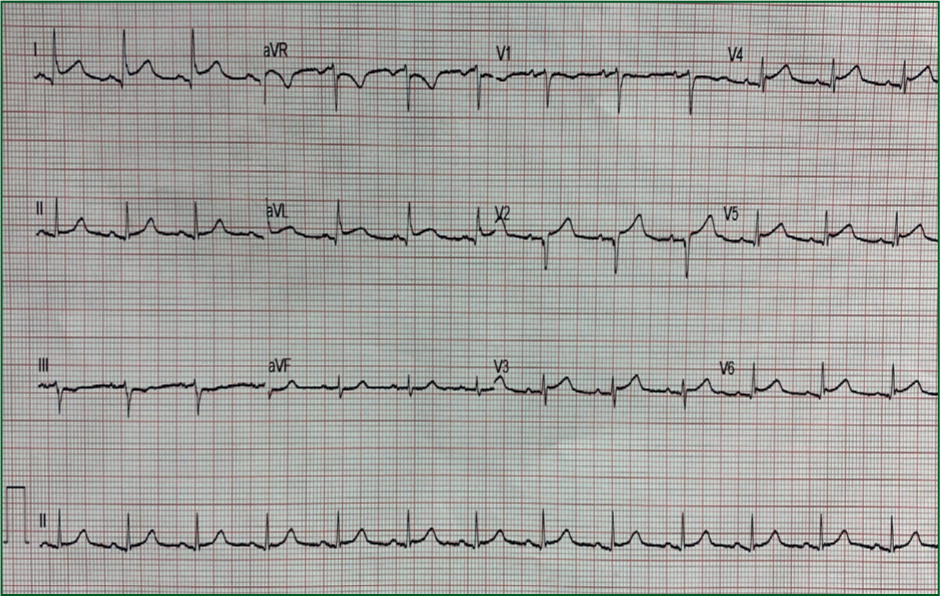
What does the ECG show?
Interpretation of the ECG rhythm
Interpretation of the 12-lead ECG
The woman was triaged to the cardiac catheterisation laboratory for emergency primary percutaneous coronary intervention. However, her coronary arteries were found to be normal. Her left ventricular gram showed classical features of Takotsubo cardiomyopathy.
Takotsubo are traditional ceramic vases that are used by Japanese fishermen to catch octopus. They have a narrow neck and wide base.
Other terminology for Takotsubo cardiomyopathy includes:
It is a condition that was first reported in Japan in 1990. It results in transient dysfunction and ballooning of the left ventricle, often triggered by a severe physical or emotional stressor, resulting in release of adrenaline and other catecholamines (about 30% have no identifiable stressor).
The left ventricle of the heart changes into a similar shape as the Takotsubo pot, developing a narrow neck and akinetic round bottom.
This condition is seen mainly in post menopausal women, often following severe stress, e.g. bereavement (‘broken heart’), assault, car accident, natural disaster, etc.
More than 90% of patients are female and 80% are aged over 50 years.
Left ventricular systolic dysfunction occurs almost exclusively. The coronary angiogram is invariably normal. Clinically, Takotsubo mimics ST segment elevation myocardial infarction (STEMI) with early ST elevation, T wave inversion and pathological Q waves.
Evaluation of left ventricular function by echocardiography usually reveals an apical zone of absent or impaired contraction. The left ventricular wall motion abnormality may return to normal within a few weeks. The outcome is usually favourable.