The clinical examination is an important part of any patient consultation. After the primary survey and taking the patient history, a more in-depth examination is sometimes required to aid making a working diagnosis and help negate other differential diagnoses. The extent of this depends on the stability of the patient and may not be possible in time-critical circumstances. However, clinical examination is an increasing part of paramedic practice owing to the continued expansion of the scope of the paramedic role in both urgent and emergency care. Education on clinical examination concerning each of the main body systems is now an integral part of undergraduate paramedic curricula.
This clinical examination series provides a step-by-step overview for each of the main body systems. Continuing professional development (CPD) is an essential requirement for all clinicians to maintain and demonstrate they are staying up to date and advancing in their roles.
This series gives an overview of each type of examination to support students, newly qualified paramedics and paramedics wishing to use these articles as a CPD development activity and an aide-memoire for clinical practice. This article, which explores the peripheral vascular system, gives an overview of initial examination considerations, including first impressions.
How to use these guides
The articles in this series, which can be torn out for use in practice, are intended to support clinician development and to assist in the overall assessment of patient presentations. The information should be used to aid consideration of differential diagnoses in situations where life-threatening conditions have been ruled out.
The extent and explanation of each examination will not be to the depth of those provided in core literature texts, so further reading and consolidation are advised to support understanding supplemental to these articles. Key questions are included for reader consideration and to direct further study.
Most examinations are taught in a rigid format. However, in clinical practice, practitioners need to be flexible and adapt their approach depending on the presenting condition and circumstances. While there is no single set way to carry out each of these examinations, a good structure will reduce omissions and errors, and support the gathering of information to inform patient care.
Contemporary texts provide the underpinning reference sources throughout this series, as many of the examination processes and techniques are universally applied; however, differences will be highlighted. Readers will be signposted to these key texts for each clinical examination.
The series will cover the following systems:
Cardiovascular system
Peripheral vascular system
Neurological system (upper and lower limbs)
Cranial nerves
Gastrointestinal system
Respiratory system
Musculoskeletal system
Peripheral vascular examination
This issue explores the peripheral vascular system and its assessment. It follows last month's article, which covered the cardiovascular system (Dearnley-Lane, 2020), and will not repeat the examinations already discussed, such as the radial, brachial and carotid pulses.
A peripheral vascular examination is indicated as part of the cardiovascular examination. Whether all aspects of the examination are assessed will depend not only on the patient's symptoms and signs, but also on the examiner's role and scope of practice.
Some aspects are fundamental to the prehospital field, while others are more pertinent to primary or urgent care roles. You need to consider whether a full examination is necessary or could be delaying you on scene.
The peripheral vascular system can be divided into the peripheral arterial system and peripheral venous systems, and the blood flow in either system may be impaired at any time by acute or chronic causes.
With this examination, you are looking for signs of vascular disease and all observations need to be taken in context with the other signs and symptoms present. Each limb should be inspected and compared with the opposite, starting with the unaffected limb.
Explain to the patient what you are going to do, gain consent and follow the guidance and considerations explained in the first article of this series (Kirk, 2020).
Physical examination
The optimal position for examination of the peripheral vascular system is for the patient to be recumbent
Abdomen
Observe for any visual pulsation above and to the left of the umbilicus. A pulsation may be visible but this is not always a concern in slimmer people
Palpate and, using a stethoscope, listen to the vertical midline of abdomen above and below the umbilicus
Palpate the aorta by placing your palms on the abdomen, with the index finger on either side of the aorta (Anderson, 2015a)
Consider an abdominal aortic aneurysm (AAA) if a lateral pulsatile mass, shown by a widening between the fingers, can be felt above the umbilicus
Consider an iliac aneurysm if a pulsatile mass can be felt below the umbilicus
Listen for bruits—turbulent blood flow within the vessel.
Lower limbs
Feel for pulses, starting distally. In the absence of a pulse, the feeding artery should be examined. For example, if you are unable to palpate a dorsalis pedis pulse, the popliteal artery may be compromised, so feel for the next pulse point, which is the popliteal pulse (College of Paramedics and American Academy of Orthopaedic Surgeons, 2016)
Inspect the legs and feet for colour changes and mottling, oedema, swelling, varicosities and ulceration/gangrene (Gregory and Ward, 2010)
Palpate for temperature differences and capillary refill
Record any pain
Note any surgical scars, particularly in the femoral triangle, along the femoral artery and in the popliteal fossa.
REFLECTION
Consider the implications of the presence/absence of the above findings during an examination
Pulses
Femoral pulse
Reconfirm consent for the procedure, ensuring discretion and dignity by avoiding unnecessary exposure
Using your index and middle fingers together, pointing upwards and slightly medially, palpate the femoral artery in the femoral triangle, halfway between the pubic tubercle and the anterior superior iliac spine. This may be difficult to feel in patients who are obese or muscular (Anderson, 2015b) and requires practice.
Popliteal pulse
Using both hands, flex the knee to approximately 30°
Place the thumbs on the patella of the knee and, with the fingers behind the knee, press firmly in the midline to palpate the popliteal artery. If you are unable to feel the pulsation, slide the fingers 2–3 cm below the knee crease to compress the artery against the back of the tibia (Grubb et al, 2013)
Popliteal pulses are difficult to feel as they lie deep in the popliteal fossa and are surrounded by large tendons (Thomas and Monaghan, 2014), so greater pressure may be required (Anderson, 2015b).
Posterior tibialis
This can be palpated with the index and middle fingers 2 cm below and 2 cm behind the medial malleolus (Ryjewski, 2015).
Dorsalis pedis
Use the pads of your middle fingers to feel one-third of the way down the middle of the superior surface of the foot, lateral to the extensor hallucis tendon (Grubb et al, 2013), between the bases of the first and second metatarsals.
REFLECTION
Why should you not press too firmly when taking a pulse?
Inspect
Is the colour the same in both legs? Is there mottling? Mottling in both legs could indicate a leaking AAA or a saddle embolus
Is there any obvious swelling to the legs? How high does the swelling extend? Is there any sacral oedema? Be aware that swelling into the groin can cause outflow obstruction in men (Thomas and Monaghan, 2014)
Using the fingertips, press gently above the ankle, medially, for 5 seconds and note any pitting (temporary indentation) (Gregory and Ward, 2010)
Are there any ulcers? These can be arterial or venous and exacerbated by infection
Compare the temperature of the limbs. Are they warm or cold?
A cold limb may indicate acute limb ischaemia, which is time critical and can be remembered using the six Ps: pulseless, pallor, perishing cold, parasthesia, paralysis and pain (Grubb et al, 2013). Consider completing a Buerger's test (described on the following page)
A warm limb may indicate deep vein thrombosis
Identify and record the location of any pain.
REFLECTION
What is the difference between an embolic versus a thrombotic acute limb ischaemia? What are the risk factors for a deep vein thrombosis?
Specialised tests
These tests are not normally performed in the prehospital field but may be undertaken in other settings within a clinician's scope of practice and training.
Arterial
Ankle:brachial pressure index
The ankle:brachial pressure index (ABPI) is a sensitive marker of arterial insufficiency and is beneficial and more reliable for patients with obesity or oedema (Grubb et al, 2013).
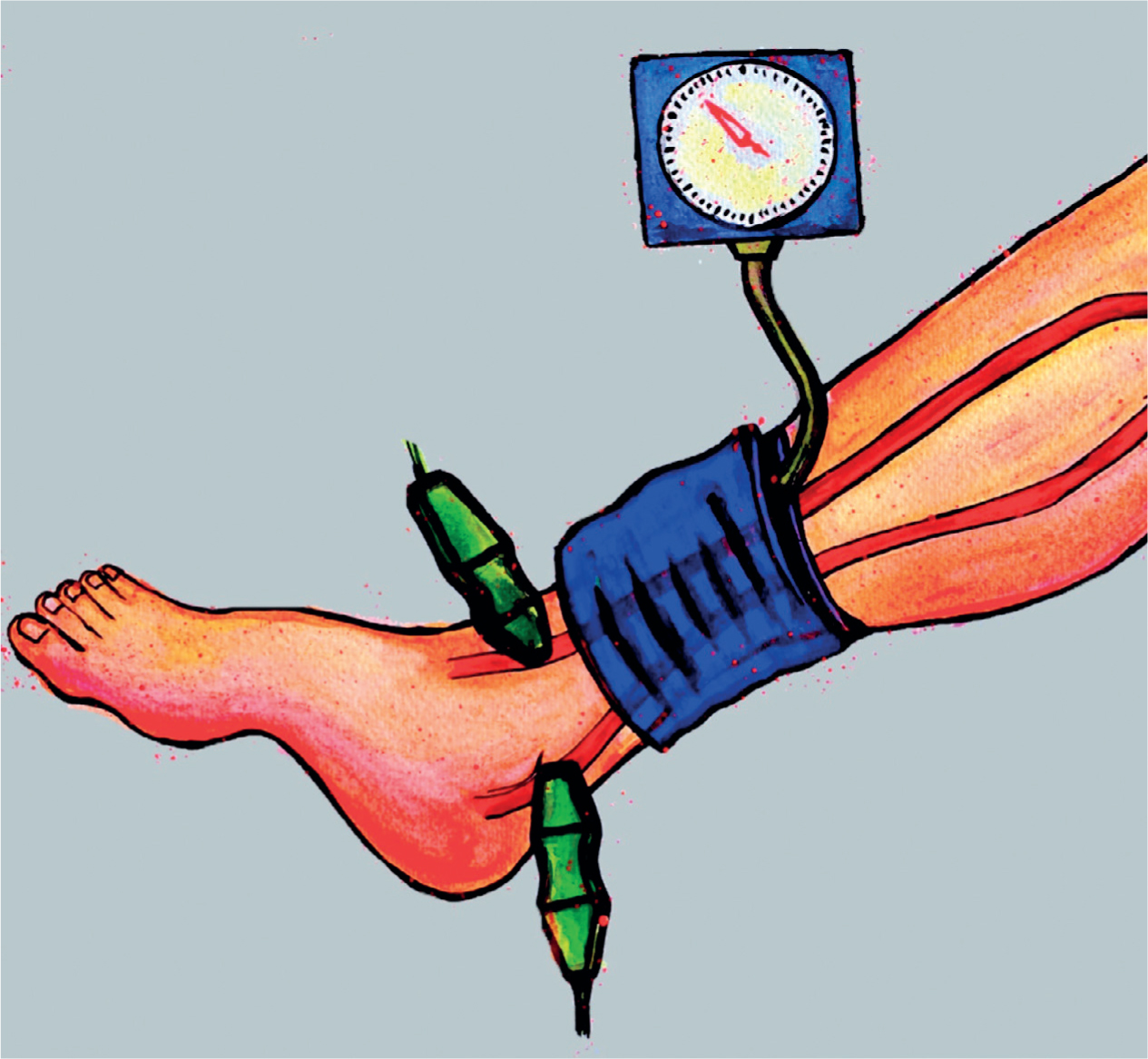
A Doppler probe is held over the pedal artery while a blood pressure cuff is inflated around the ankle (Figure 1), and the pressures recorded when the Doppler signal disappears. This is repeated over the posterior tibial artery
The brachial blood pressure is measured as normal
The normal systolic blood pressure in the legs is the same or greater than that in the arms so a normal ABPI should be ≥1 in the supine position. Readings below this suggest a level of claudication.
Figure 1. Systolic blood pressure is recorded in the arteries of the ankle after each arterial flow is located
REFLECTION
What is claudication? Describe the difference between pain that comes and pain that comes on during exertion
Buerger's test
With the patient lying supine, stand at the foot of the bed, raise and support the legs at 45° for 2–3 minutes and look for extreme pallor of the feet and guttering (emptying) of the superficial veins (Grubb et al, 2013)
Blood flow and colour will return; in a positive test, the skin initially becomes blue, because the blood is deoxygenated as it passes through the ischaemic tissue, then red, because of reactive hyperaemia, from post-hypoxic vasodilation
Examine both limbs simultaneously, as pallor and redness are positive signs of a Buerger's test, indicating critical limb ischaemia, and are most obvious when one leg has a normal circulation.
Allen test
This tests the collateral blood flow to the hand before taking radial arterial bloods or arterial cannulation to avoid risk of hand ischaemia, so is not used in the prehospital environment (Anderson, 2015b).
Venous
Trendelenberg test
Here, varicose veins are examined to evaluate venous insufficiency and competence of the saphenofemoral junction in the femoral triangle and of the perforator veins between superficial and deep venous systems (Anderson, 2015b).
On completion of the examination, thank the patient and document your findings. Reflect on your examination and consider what abnormal findings may mean in the context of the patient's overall presentation.
Remember to only perform examinations within the parameters of your scope of practice and training.
This concludes the examination of the peripheral vascular system. Next month's issue will examine the musculoskeletal system.