
Timely acquisition of reliable vascular access is essential for the delivery of both drugs and fluids for critically unwell patients (Lewis and Wright, 2015). In practice, however, this is frequently difficult as peripheral veins can collapse during hypovolaemia and haemorrhage (Anson, 2014). Additionally, the degree of urgency in which vascular access is required is often directly proportional to the difficulty of the insertion (Lewis and Wright, 2015).
Intraosseous (IO) access uses the rich, non-collapsible vascular system within the bone marrow cavity to overcome many of the problems faced by clinicians (Rosenberg and Cheung, 2013). The success of this approach has led to its widespread adoption within many guidelines as a standard approach when traditional peripheral intravenous (IV) access is difficult or impossible (Maconochie et al, 2015; Nolan et al, 2016).
Despite the popularity and use of IO access in emergency care, administration of large volumes of fluid is difficult because rates are slow compared with when IV cannulas are used (Pasley et al, 2014). From an anatomical perspective, the primary reason for this difference is the mean blood pressure of 20–30 mmHg in the medullary space; when coupled with the presence of bone spicules (which remain following the initial flushing), it increases flow resistance between the bone cavity and vascular system (Anson, 2014; Petitpas et al, 2016). Other factors that commonly affect flow rates include:
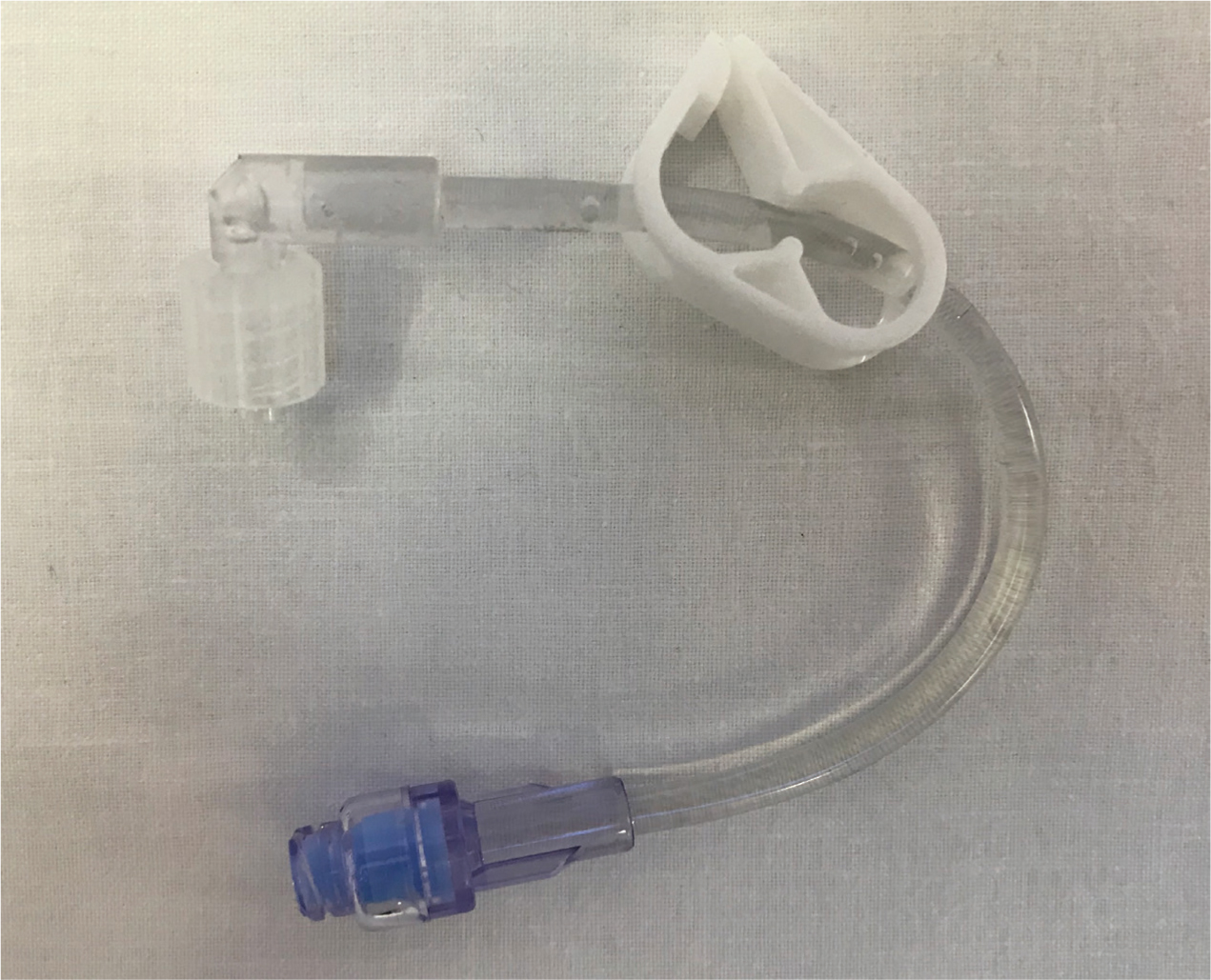
The EZ-IO device (Teleflex Medical, Athlone, Ireland) is commonly employed by clinicians in the UK. Each single-use needle packet contains the company's adapter, which includes a needle-free port. A study by Reddick et al (2011) has previously demonstrated that needle-free connectors resulted in flow rates that were up to 40% slower than when a selection of peripheral IV access devices was used. The effect of the manufacturer extension set on IO flow rates has not been documented in the literature. It is postulated that it may be possible to improve flow rates by using different methods.
Methodology
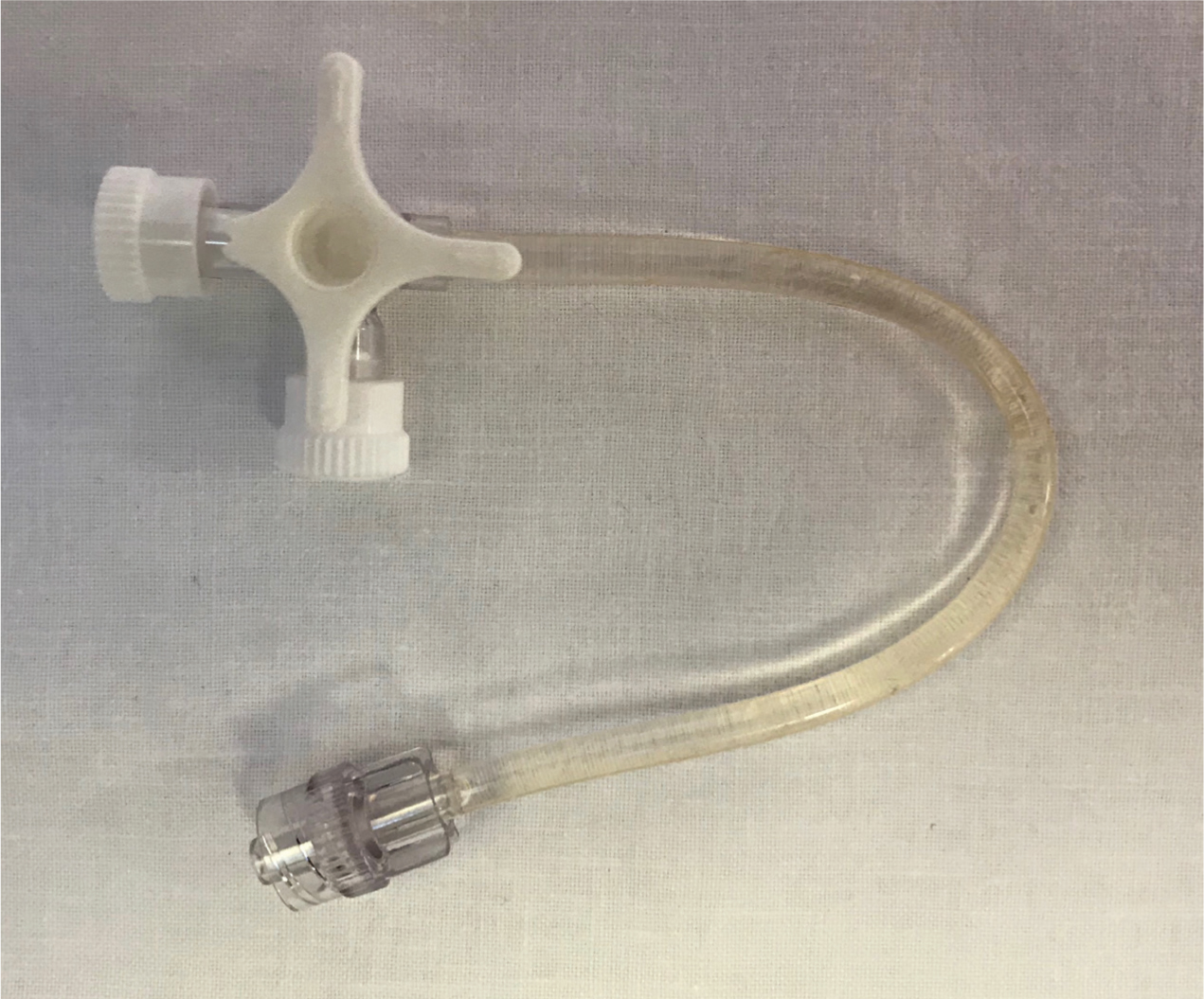
Three different methods of administration were examined:

The null hypothesis was that all administration methods would be equal. Thirty experiments were conducted using a randomisation schedule (with blocks of 10), and the time taken for 500 ml of 0.9 % saline to be administered through a 15 ga EZ-IO needle was recorded. This was conducted under free drainage (without a pressure bag). A standardised 50 cm drop height was used for all fluid bags. The time keeper was blinded to the method of administration. Blinding was maintained until statistical analysis had been completed.
While ethical approval was considered, it was not felt to be required as the study was an examination of devices only and did not directly involve any patients or staff members.
Results
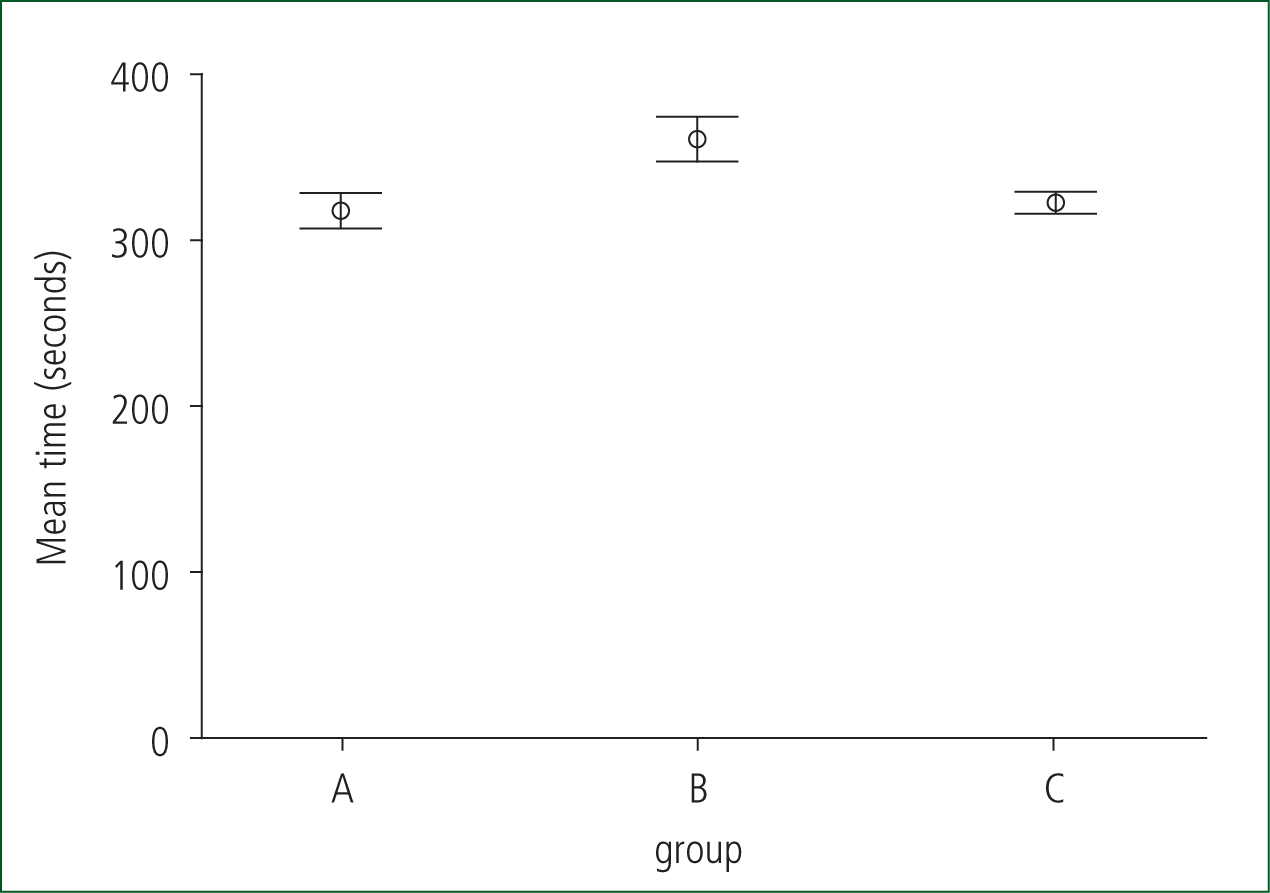
Methods A (DTH), B (EZS) and C (TWS) had a mean time of 317.8 s (SD 15.06), 361.1 s (SD 19.12) and 322.7 s (SD 8.3) respectively (Table 1; Figure 4). The flow rates were therefore calculated to be 94.5 ml/minute (DTH), 83 ml/minute (EZS) and 93.1 ml/minute (TWS).
| Group | Mean(s) | n | SD |
|---|---|---|---|
| A: DTH | 317.8 | 10 | 15.06 |
| B: EZS | 361.1 | 10 | 19.12 |
| C: TWS | 322.7 | 10 | 8.30 |
| Total | 333.9 | 30 | 24.36 |
An analysis of variance (ANOVA) test was conducted using SPSS software (v. 24) to adopt or reject the null hypothesis. There was a difference between the three groups (ANOVA p<0.0001) and hence the null hypothesis can be rejected (Table 2).
| Sum of squares | df | Mean square | F | Sig | ||
|---|---|---|---|---|---|---|
| Time * group | Between groups (combined) | 11 261.795 | 2 | 5630.897 | 25.545 | p<0.0001 |
| Within groups | 5951.600 | 27 | 220.430 | |||
| Total | 17 213.395 | 29 |
Discussion
This in-vitro study, which controlled for type of fluid, height of the bag, giving set and needle gauge, has demonstrated that there are statistically significant time differences between these three methods of administration through an IO needle. The slowest method was the extension set that is provided with the EZ-IO needle, which took a mean of 361.1 s to infuse 500 ml of 0.9% saline. DTH and TWS were 12% and 10.6% quicker respectively, which are equivalent to respective higher flow rates of 11.5 ml/minute and 10.1 ml/minute.
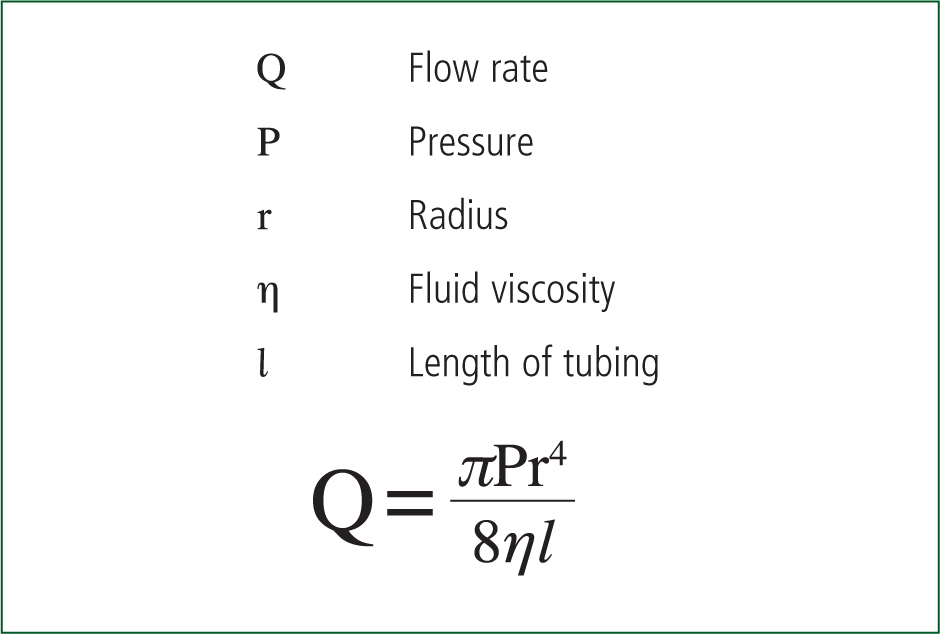
Poiseuille's law (Figure 5) shows that the flow of fluid in a tube is directly proportional to the radius (to the power of 4), and is inversely proportional to its length (Reddick et al, 2011). This principle implies that a long, narrow tube will have a slower flow rate than a short, wide one. While this is important when choosing a vascular access device, other factors will influence the flow rates that can be achieved. Needle-free devices (e.g. on the EZ-IO extension set) are increasingly popular and have the desirable aim of decreasing spillages and needlestick injuries, alongside the avoidance of touch contamination (Reddick et al, 2011). This device does appear, however, to increase the flow resistance through the IO needle, although the effect is less profound than those demonstrated in IV catheters (Reddick et al, 2011).
One weakness of the present study is that it is unclear if this effect would occur in real patients; intuitively; however, it appears that the principle should still apply. Further work will seek to inform this area of practice.
In clinical practice, it is commonplace for IO flow rates to be improved with the use of pressure bags or by manually infusing 50 ml boluses via a three-way tap. These methods were not examined during the current study and using them may alter the results and effect size. The authors suggest that the TWS approach would enable both of these methods to continue to be used (but with the additional 10.6% increased flow), providing optimum flow rates where large or rapid infusions are required.
Conclusion
This study has demonstrated the potential to improve IO flow rates by 12% or 11.5 ml/minute through simply changing the extension set used for fluid infusion. In practice, the use of a TWS with a pressure bag and/or manual infusion of fluids is likely to increase the rate of fluid administration through IO needles.